
by Susan Coppa, Stanford University

Credit: Pixabay/CC0 Public Domain
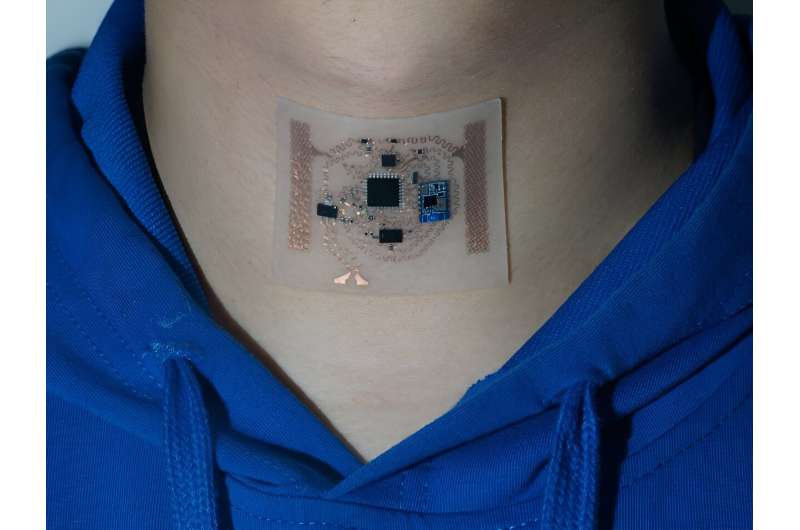
Brian Suffoletto, MD, associate professor of emergency medicine, views interactions with patients in the Emergency Department as valuable opportunities to identify specific risks and then facilitate positive behavior changes post-ED discharge using digital devices.
He has spent more than 10 years developing digital behavioral interventions for various medical risks from young adult binge drinking to distracted driving.
In this Q&A, we asked Suffoletto about his work and research into digital tools that can both recognize and address the negative impact alcohol use can have on a person's health.
Many of your studies explore how digital devices can detect and reduce adolescent intoxication and binge drinking. Why did you choose to focus on this area?
Two of my close friends died in an alcohol-related car accident when I was in college. I also worked for many years in an inner-city hospital in Pittsburgh with a large referral base of young adults from various colleges, so I saw a lot of alcohol-related injuries and conditions in the emergency department.
Emergency medicine physicians have traditionally used a method called Screening, Brief Intervention and Referral to Treatment (SBIRT) that employs motivational interviewing techniques to try to persuade individuals to reduce their drinking.
But we rarely have the time or setting to effectively address the impact of alcohol use on a patient's health. In addition, emergency department patients are often distracted, in pain or even intoxicated, so receptivity to those messages is low.
I started exploring using digital technology, including text messaging to reach people in small but repeated ways to influence health behaviors over time. With this approach, I was no longer constrained by the limitations of the hospital walls. I could, instead, identify emergency department patients at risk, then communicate with them afterward to try to influence their everyday decisions.
Can you describe recent machine modeling you and collaborators from the University of Toronto employed to predict intoxication based on measurable changes in voice?
Fluent speech depends on the rapid and precise coordination of more than 100 muscles orchestrated by high-level sensory, cognitive, and motor processes. So, you can evaluate a person's voice on things like phonation (breathy, guttural, or creaky voice), pitch, loudness, rate, and other variables.
This study focused on frequency-based voice features—how loud a voice is—as these are particularly good at demonstrating levels of intoxication. We used tongue twisters because they act as a stress test, revealing even subtle disruptions in this intricate coordination system. Then, based on those measurable changes in voice, we built a model that predicted alcohol intoxication with an accuracy of 98%.
Tell us about the text message interventions to reduce alcohol consumption.
The best time to intervene is often prior to the behavior but soon enough to be contextually relevant. For instance, as someone starts drinking, a reminder of their consumption limits can be impactful. However, once a person is significantly intoxicated, these interventions are less effective. So, in one study we use collected voice data to identify the best time to intervene and then develop text messaging tools to help reduce risky drinking.
What advantages do digital devices offer in spurring behavioral change?
The reality is that we don't always have someone to steer us away from bad life decisions and behaviors.
However, we are almost constantly tied to digital devices, primarily cell phones but also new wearables, so it seems natural to use these technologies to reach people.
There are two components to interventions—frequency and intensity. The whole idea behind just-in-time interventions is that we can identify periods of risk or opportunities for certain behavior, then use digital devices to nudge a person in the direction of healthy behavior at optimal moments.
It seems there is no magic formula for content in those digital nudges; it's actually less about content and more about timing that can assist someone in self-monitoring. By being brief and focusing on short-term goals, we enable people to use their own intrinsic motivation, which is much more effective than lecturing.
You used smartphone accelerometer sensors to detect alcohol intoxication by analyzing an individual's gait. How effective is a smartphone at detecting intoxication?
I've led several research projects to detect alcohol consumption remotely through digital biomarkers, analyzing GPS-tracked mobility, texting speed and errors, and gait patterns. In one gait analysis study, we had participants walk 20 steps with smartphones placed on their backs to record accelerometer data.
Then they drank enough alcohol to reach a breath alcohol concentration of 0.20% and repeated the same walk over subsequent hours, while we measured gait changes using the accelerometer data. We could accurately identify a breath alcohol concentration of greater than 0.08% more than 92% of the time.
How has this work evolved over time?
Using technology to influence behaviors is a double-edged sword. On one hand, an individual can influence a lot of people at once, and automated systems can have broad geographic reach. On the other hand, people's expectations for how technology should look, and function are rapidly changing because of large language models and the advancements in chatbot technology.
It's harder to retain the attention of the average individual through electronic mediums than it was 10 years ago, and new messaging modalities constantly pop up. However, text messaging use has remained constant over time and presents many opportunities to change health behaviors and hopefully help patients after they leave the emergency department.
Provided by Stanford University






Post comments