
by Thamarasee Jeewandara , Medical Xpress
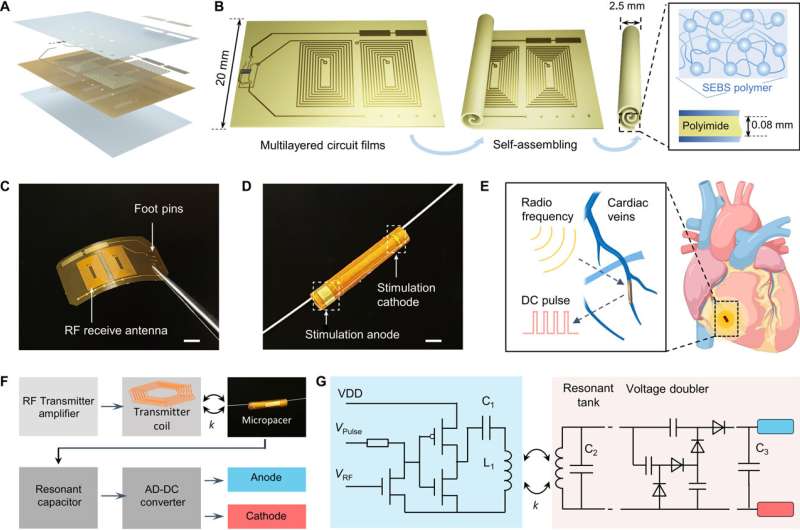
The implantable microtubular pacemaker for wireless pacing. (A) Multilayered circuit film for the microtubular pacemaker includes the following layers, arranged from bottom to top: SEBS encapsulation, polyimide film, circuits and components, SEBS encapsulation, and gold stimulating electrodes. (B) A schematic diagram of the microtubular pacemaker is fabricated by a self-assembling process, which benefits from the self-adhesiveness of SEBS polymer layer. (C) An optical image of an f-PCB film, which shows the two RF receiver antenna and foot pins for microcomponents. Scale bar, 5 mm. (D) An optical image reveals a guide wire through the microtubular pacemaker. The stimulation cathodes and anode are shown in the white dashed box. Scale bar, 2 mm. (E) A schematic illustration highlights the implantation of the microtubular pacemaker to the cardiac anterior vein. The microtubular pacemaker receives the RF wirelessly and generates DC pulses to stimulate the heart. (F) An operational diagram illustrates the wireless intravascular pacing system, where the external transmitter device generates inductive power transfer to the receiver coils of the pacemaker for electrical stimulation. (G) The circuit diagram of the portable RF transmitter (light blue background) and the implantable microtubular pacemaker (light orange background). VDD, Voltage Drain to Drain. Credit: Science Advances, doi: 10.1126/sciadv.adj0540
Cardiac pacemakers are battery-dependent, where the pacing leads are prone to introduce valve damage and infection. In addition, complete pacemaker retrieval is necessary for battery replacement. Despite the presence of a wireless bioelectronics device to pace the epicardium, surgeons still need to implant the device via thoracotomy, an invasive surgical procedure in health care that necessitates wound healing.
Shaolei Wang and a research team of scientists in bioengineering, microbiology, and cardiology at the University of California, Los Angeles, devised a biocompatible wireless microelectronics device to form a microtubular pacemaker for intravascular implantation and pacing. Their wok has been published in Science Advances.
The pacemaker provided effective pacing to restore cardiac contraction from a non-beating heart in a porcine animal model. The microtubular pacemaker paves the way for the minimally-invasive implantation of leadless and battery-free microelectronics for health care and cardiac pace restoration.
Advances in vascular surgery
Microstimulators can be implanted as cardiac, gastric, neural, and urological devices to sustain life. While pacing leads are prone to discharge, fracture and biofilm formation, the effort to generate leadless pacemakers that are battery-free for minimally invasive implantation remain an unmet challenge in biomedical engineering.
Advances in catheter-based deployment for biomedical implants include bioprosthetic valves. In this work, Wang and colleagues established a self-assembled, implantable, microtubular pacemaker made of lightweight and wireless constituents, to provide high electrical output and operational capacity to facilitate intravascular myocardial pacing and mechanical coupling.
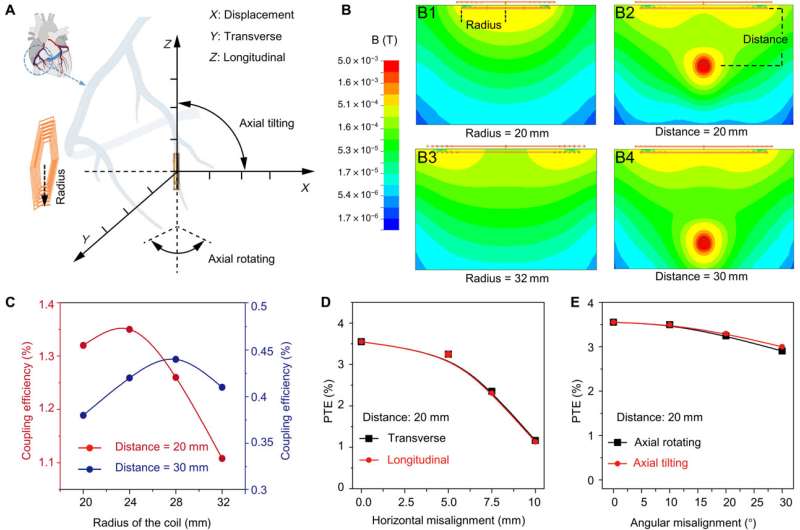
Simulation of coupling efficiency for inductive power transferring. (A) A schematic diagram reveals the displacement, misalignment (transverse direction and longitudinal direction), and angular misalignment that may affect the PTE. (B) (B1 and B3) Magnetic fields were simulated at various radii of the transmitter coil (r = 20 to 32 mm). (B2 and B4) The coupling efficiency was dependent on the displacement ranging from 20 to 30 mm. (C) The coupling efficiency as a function of radius of the coil was compared between the distance of 20 and 30 mm. (D) There is a correlation in PTE as a function of horizontal misalignment from 0 to 10 mm between the transverse and longitudinal direction. (E) There is also a correlation in PTE as a function of angular misalignment from 0o to 30o between axial rotation and tilting. Credit: Science Advances, doi: 10.1126/sciadv.adj0540
Forming a self-assembled, microtubular pacemaker
The team accomplished this by designing a microtubular pacemaker to reduce the mechanical burden of pacing-related medical complications. They generated a wireless radiofrequency module in a thin, flexible polyimide membrane to receive power transfer from the external transmitter. They encapsulated the polyimide membrane with an elastomer layer to insulate the circuits and optimized power transfer efficiency to the microtubular pacemaker by designing a radiofrequency power transmitter for electrical stimulation.
After implanting the device in the anterior cardiac vein, the scientists demonstrated the capacity of the microtubular device to re-energize the non-beating heart, recorded via cardiac electrocardiograms to restore myocardial contraction and perform wireless, and leadless myocardial stimulation.
Designing the self-assembled microtubular pacemaker
The scientists designed the self-assembled microtubular electronics to suit the cardiovascular anatomy and electrophysiology for wireless and battery-free stimulation.
The team illustrated the concept to facilitate intravascular implantation, where the flexible printed circuit board membrane contained a pair of antennas, a rectifier circuit and anode/cathode electrodes to deliver the direct current pulses for myocardial stimulation. The team designed the smaller electrodes to maintain an optimal current density to reduce power consumption during cardiac stimulation. The setup stored the direct current energy before delivering direct current pulses to the anode and cathode electrodes.
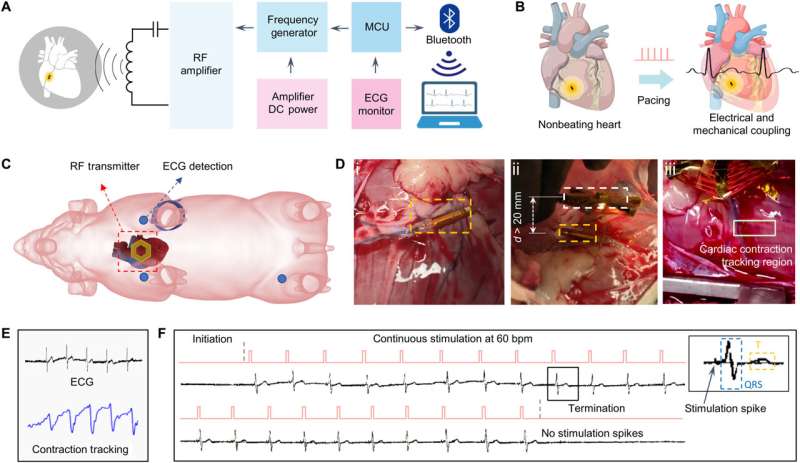
Intravascular implantation of the microtubular pacemaker to restore cardiac conduction and myocardial contraction. (A) A schematic illustrates the portable system combining an RF transmitter and an MCU to achieve wireless power delivery and ECG data acquisition. (B) Intravascular implantation of the microtubular pacemaker to the anterior vein of a nonbeating heart. Induction of transmitter coil for magnetic interaction with the receiver coil. (C) RF transmitter coil is placed above the epicardium where the microtubular pacemaker is implanted to the ACV in an anesthetized pig. The ECG pads were connected to the left upper limb, right upper limb, and left lower limb. (D) (Di) Implantation of the microtubular pacemaker in the ACV. (Dii) Displacement between external transmitter (white dashed box) and the microtubular pacemaker (orange dashed box) was greater than 20 mm for inductive power transferring. (Diii) Myocardial contraction was recorded by the video tracking of an epicardial region of the left ventricle. The contraction region was labeled, and the moving coordinates around the center of the region were calibrated to synchronize with the ECG. (E) Video tracking of myocardial contraction in response to electrical stimulation. (F) ECG rhythm strip reveals the initiation of electrical stimulation in the nonbeating heart at 60 bpm as evidenced by the consistent pacing spikes, followed by QRS for myocardial activation and T waves for repolarizations (inset). Removal of the RF transmitter coil terminated the stimulation spikes. Credit: Science Advances, doi: 10.1126/sciadv.adj0540
Optimizing the efficiency of the pacemaker through magnetic field stimulation
The scientists optimized the power transfer efficiency through magnetic field stimulation from the transmitter coil to the receiver coil using the ANSYS software. They noted the maximum strength of the magnetic field to occur in the region proximal to the transmitter coil.
Myocardial contraction typically generates a periodic misalignment around the original position during a cardiac cycle. As a result, the alignment of the transmitter and receiver coil influenced the efficiency of inductive powering transferring.
The team studied the strength of the inductively powered system through in vitro testing, where the initiation and termination of radiofrequency pulses were coupled to the direct current pulses. They used a two-circuit architecture to compare radiofrequency alternate current, direct current conversion with a full bridge rectifier, to provide a sufficient energy threshold to re-energize the non-beating heart of a porcine animal model.
Using electrical impedance spectroscopy, Wang and colleagues studied the electrical impedance and phase of the stimulating electrodes.
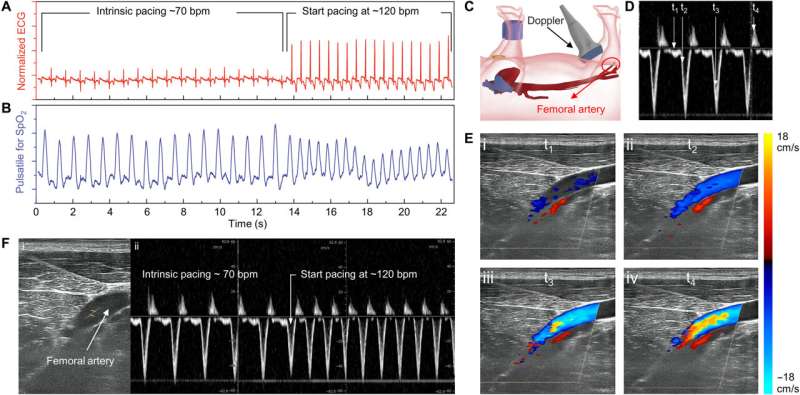
Intravascular implantation of the microtubular pacemaker to restore hemodynamic blood flow. (A and B) ECG and SpO2 monitoring in response to cardiac contraction from 70 to 120 bpm. (C) The schematic illustrates the placement of duplex ultrasound to detect blood flow from the femoral artery. (D) Pulsed wave Doppler detected the pulsatile arterial blood flow in response to cardiac contraction. (E) t1 to t4 indicate the Doppler signals at different cardiac cycles. t1 corresponds to diastole, t2 corresponds to early systole, t3 corresponds to mid-systole, and t4 corresponds to end systole. The color gradients indicate the direction and magnitude of blood velocity toward the hindlimb. (F) Pulsed wave Doppler detected femoral arterial blood flow in response to cardiac pacing from 70 to 120 bpm. Credit: Science Advances, doi: 10.1126/sciadv.adj0540
Outlook: Biocompatibility of the microtubular electronics
The team tested the biocompatibility of the materials by using an in vitro incubation assay and included peripheral blood mononuclear cells (PBMCs) to investigate the surface-biocompatibility and inflammatory response of a variety of materials. The constituent population of PBMCs included granulocytes, monocytes, and lymphocytes that actively triggered inflammation and an immune response upon exposure to a biomaterial.
When the bioengineers incubated the blood cells with materials used in the microtubular pacemaker, they noted the absence of cell toxicity and immune responses for up to a week. The constructs showed hemocompatibility and immunogenicity in the microtubular pacemaker.
In this way, the scientists further explored intravascular pacing to restore electromechanical coupling and blood circulation. The porcine heart models resembled human physiology suited for clinical translational in vivo studies.
The team recorded myocardial contraction relative to electrical stimulation as epicardial movements.
The self-assembled microtubular pacemaker provided an innovative method for intravascular deployment with translational impact in cardiac, gastric, and urological stimulations; eliminating the need for a charge storage unit in bioelectronics, with suitability for open-chest thoracotomy and to accelerate wound healing post-implantation.
More information: Shaolei Wang et al, A self-assembled implantable microtubular pacemaker for wireless cardiac electrotherapy, Science Advances (2023). DOI: 10.1126/sciadv.adj0540
Journal information: Science Advances
© 2023 Science X Network








Post comments