
by The Peter Doherty Institute for Infection and Immunity

VRE bacteria on a petri dish and Rifaximin antibiotics. Credit: Adrianna Turner
A new study has found that an antibiotic for liver disease patients could expose them to greater risk of a dangerous superbug.
The international team of researchers found that an antibiotic commonly prescribed for patients with liver disease, called rifaximin, has led to the global emergence of an almost untreatable form of the antimicrobial resistant superbug vancomycin-resistant enterococcus faecium (VRE), which frequently causes serious infections in hospitalized patients.
The study has demonstrated that rifaximin usage is driving resistance to daptomycin, one of the last effective antibiotics against VRE infections.
Published Oct. 23 in Nature, the study was led by researchers from the University of Melbourne at the Peter Doherty Institute for Infection and Immunity (Doherty Institute) and Austin Health and highlights the critical need for a deeper understanding of the negative impacts of antibiotic use—reinforcing the importance of responsible antibiotic use in clinical practice.
Their findings reinforce the recent political declaration of the UN General Assembly High-Level Meeting on Antimicrobial Resistance (26 Sept 2024), where world leaders committed to decisive action on antimicrobial resistance, including reducing the estimated 4.95 million AMR-associated human deaths annually by 10% by 2030.
The eight-year study drew on several disciplines, including molecular microbiology, bioinformatics and clinical science. Using large-scale genomics—the study of an organism's DNA makeup—the scientists were able to identify changes in the DNA of daptomycin-resistant VRE that were absent in susceptible strains. Subsequent laboratory experimentation and clinical studies showed that rifaximin use caused these changes and resulted in the emergence of daptomycin-resistant VRE.
The University of Melbourne's Dr. Glen Carter, a senior research fellow at the Doherty Institute and senior author of the study, said the research challenges the long-held belief that rifaximin poses a "low risk" for causing antibiotic resistance.
"We've shown that rifaximin makes VRE resistant to daptomycin in a way that has not been seen before," Dr. Carter said.
"It is also of concern that these daptomycin-resistant VRE might be transmitted to other patients in the hospital; a hypothesis that we are presently investigating."
The University of Melbourne's Dr. Adrianna Turner, a Research Officer at the Doherty Institute and first author of the study, said rifaximin triggers specific changes in an enzyme called RNA Polymerase within the bacteria. These changes "upregulate" a previously unknown gene cluster (prdRAB) leading to alterations in the VRE cell membrane and causing cross resistance to daptomycin.
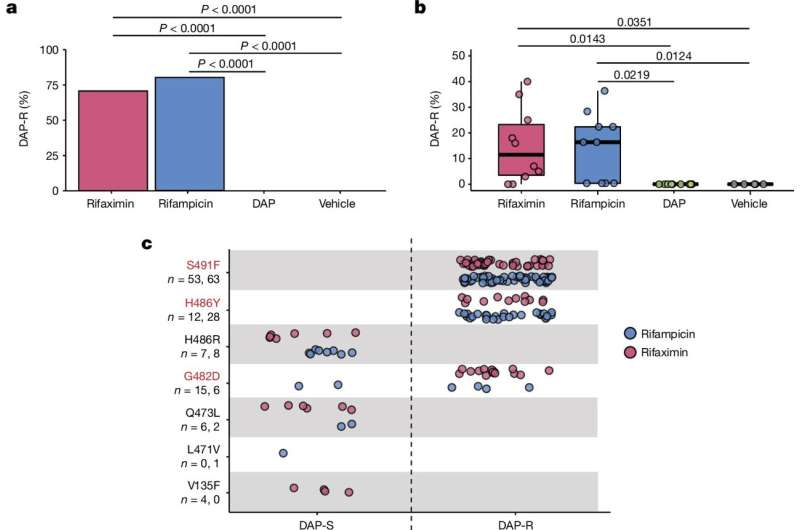
Rifaximin drives the emergence of DAP-R VREfm. Credit: Nature (2024). DOI: 10.1038/s41586-024-08095-4
"When bacteria become resistant to an antibiotic, it's a bit like gaining a new ability in a video game, like super-speed. But when exposed to rifaximin, the VRE bacteria don't just get one boost—they gain multiple abilities, like super-speed and super-strength, allowing them to easily defeat even the final boss, which in this case is the antibiotic daptomycin," Dr. Turner said.
"In other words, rifaximin doesn't just make bacteria resistant to one antibiotic; it can make them resistant to others, including critical last-resort antibiotics like daptomycin."
Associate Professor Jason Kwong, infectious diseases physician at Austin Health and lead investigator of the clinical studies, emphasized two critical implications of the findings.
"Firstly, clinicians must exercise caution when treating VRE infections in patients who have been taking rifaximin, since daptomycin's efficacy may be compromised, necessitating laboratory verification before use," Associate Professor Kwong said.
"Secondly, the findings underscore the importance of regulatory bodies considering 'off-target and cross class' effects when approving new drugs. For antibiotics, this means understanding whether exposure to one agent, like rifaximin, could induce resistance against other antibiotics—even those that work differently.
"Rifaximin is still a very effective medication when used appropriately and patients with advanced liver disease who are currently taking it should continue to do so. But we need to understand the implications going forward both when treating individual patients and from a public health perspective."
The University of Melbourne's Dr. Claire Gorrie, a senior bioinformatician from the Doherty Institute and co-senior author, said the research highlights how cutting-edge technologies, combined with interdisciplinary collaboration, can uncover exactly how and why bacteria develop resistance to antibiotics—even those they've never encountered.
"These insights are crucial for developing smarter, more sustainable strategies for antibiotic use, especially as these life-saving drugs become an increasingly precious resource," Dr. Gorrie said.
Professor Benjamin Howden, the director of the Microbiological Diagnostic Unit Public Health Laboratory at the Doherty Institute and an Infectious Diseases Physician at Austin Health, whose laboratory led the project, said the research will help ensure daptomycin remains an effective antibiotic for treating severe VRE infections in hospitals in Australia and around the world, particularly in the most vulnerable patients.
"Our findings highlight the critical need for effective genomics-based surveillance to detect emerging antimicrobial resistance. They also underscore the importance of judicious antibiotic use to safeguard vital last-resort treatments like daptomycin," Professor Howden concluded.
More information: Adrianna M. Turner et al, Rifaximin prophylaxis causes resistance to the last-resort antibiotic daptomycin, Nature (2024). DOI: 10.1038/s41586-024-08095-4
Journal information: Nature
Provided by The Peter Doherty Institute for Infection and Immunity








Post comments