
by Queen Mary, University of London
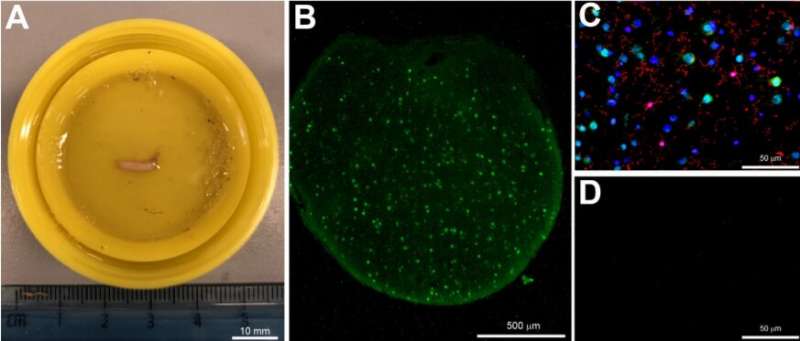
Figure 1. Cerebral biopsy sample and fluorescent immunostaining. (A) An image of the cerebral biopsy obtained from a severe TBI patient and fixed in 10% formalin. (B) A cross-section of the biopsy stained with the neuronal marker NeuN (green, ×4 magnification). (C) Biopsy stained with NeuN (green), Iba1 (red) and Hoechst (blue) (×40 magnification). (D) Negative control of immunostaining with the primary antibody omitted. Scale bars: (A), 10 mm; (B), 500 µm and (C,D) 50 µm. Credit: DOI: 10.3390/biomedicines10030518
New research led by Queen Mary University of London and Barts Health NHS Trust suggests that biochemical analysis of brain tissue could be used for diagnosis and prognosis of severe traumatic brain injury (TBI) to improve patient outcomes and save billions in future clinical trials.
The study, published in Biomedicines, is the first to look at what happens to the injured brain at a cellular and molecular level in the acute phase. The study involved 25 adult patients—with brain biopsies obtained shortly after injury undergoing specialized analysis called immunohistochemistry. This analysis revealed previously unknown cellular and biomolecular changes, allowing the researchers to 'score' the severity of injury using their own novel grading system.
TBI affects millions of patients annually worldwide and many suffer severe disability and death. It is an extremely complex disease, making the severity of injury difficult to classify.
The researchers were able to gain vital information about the type and severity of the patients' injuries, meaning that they could determine whether they might benefit from certain treatments. For example, the appropriateness of a potentially lifesaving but highly invasive surgical procedure to remove sections of the skull is currently decided on clinical acumen with little robust evidence, and immunohistochemical analysis could help guide this treatment decision. Current neuroimaging techniques such as CT and MRI lack the resolution to detect cellular and molecular changes, and the information demonstrated in this study adds significantly to the diagnostic tools available. The methods have been refined to show results within 12 hours, meaning that the information is available early on in the patient's treatment.
Co-study lead Dr. Ping Yip, senior lecturer in neuroscience at Queen Mary University of London, said: "We believe this could revolutionize the way we diagnose TBI in patients and also pave the way to finding effective treatments.
"Over the past 25 years more than $1 billion has been spent worldwide on clinical trials of more than 30 drugs and all have failed to show any benefit in severe brain injury. The likely reason, which this research is the first to demonstrate, is that brain injury is actually a range of conditions rather than a single disease. Inadvertently testing a single treatment on a range of conditions means that if a patient does benefit, they are hidden within a larger group that does not benefit as a whole, and the trial fails."
Co-study lead Dr. Chris Uff, consultant neurosurgeon and head of neurotrauma at the Royal London Hospital Major Trauma Centre, said: "A useful comparator is cancer treatment: you would not treat all cancers, regardless of their type or severity, with a single drug, and the same principle applies to brain injury. Different drugs may well improve outcome in patients depending on their injury type, and these drugs may already be available. We just need to unlock their potential with accurate diagnosis, which is where cellular and biomolecular analysis can be so useful."
Brain tumors were first classified by Percival Bailey into 13 categories in 1926, and to date the World Health Organization classifies brain tumors into 150 different types. TBI classification still relies on the Glasgow Coma Scale which was developed in 1974 and uses a simplistic 3-tier system of mild moderate and severe. This study aims to allow TBI to follow in the footsteps of neuro-oncology.
Brain biopsy is used very commonly in brain cancer diagnosis, and this study shows that it is also safe to for patients who have suffered severe TBI to undergo brain biopsy. This means that this technique can be further investigated and refined, potentially benefitting patients worldwide.
More information: Ping K. Yip et al, Characterisation of Severe Traumatic Brain Injury Severity from Fresh Cerebral Biopsy of Living Patients: An Immunohistochemical Study, Biomedicines (2022). DOI: 10.3390/biomedicines10030518
Provided by Queen Mary, University of London






Post comments