
by American College of Surgeons
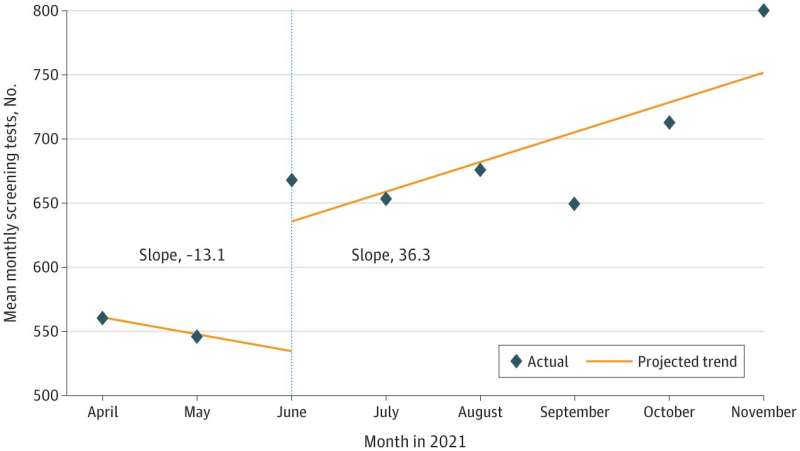
Mean Monthly Screening Test Volumes in April Through November. 2021 April and May 2021 is the preintervention period. Vertical dotted line indicates the start of the intervention period (June 2021). Credit: JAMA Network Open (2022). DOI: 10.1001/jamanetworkopen.2022.42354
A national Return-to-Screening effort initiated and led by the American College of Surgeons (ACS) helped restore cancer screenings to pre-pandemic levels and contributed to a significant number of additional screening tests, according to new research published in JAMA Network Open.
In response to growing concerns about missed cancer screenings related to COVID-19 restrictions and lockdowns, the ACS Cancer Programs, together with the American Cancer Society, launched a Return-to-Screening national Quality Improvement (QI) Project in early 2021 to help accredited programs estimate and reduce local cancer screening deficits.
The article in JAMA Network Open reveals, for the first time, final data from the QI project, which included 786 Commission on Cancer (CoC) and National Accreditation Program of Breast Centers (NAPBC) accredited programs. These programs include hospitals, treatment centers, and other cancer facilities. It is estimated that the CoC programs treat nearly 70 percent of recently diagnosed cancer patients in the U.S. annually.
The collaboration marked the first time when the accredited programs came together under one unified quality improvement goal, noted corresponding author Heidi Nelson, MD, FACS, Medical Director of ACS Cancer Programs.
"When we first started enrolling accredited programs in this quality improvement project, we discovered that more than half of the participating sites still had not returned to pre-pandemic levels of monthly screening by early 2021," she said.
"We learned that by applying a unified quality improvement framework with toolkits, collaborative learning opportunities, and other resources, we could positively increase screening rates and reverse the trends we were seeing related to missed screenings. The same principles we used here can potentially be used as a model to address other gaps in cancer care."
Accredited cancer programs are squarely focused on providing quality care for patients, Dr. Nelson added, and the environment of these programs optimally allowed centers to quickly resume screening patients across the country.
For this study, researchers established project-specific targets based on differences in mean monthly screening test volumes between pre-pandemic (September 2019, January 2020) and pandemic (September 2020, January 2021) time periods. Between June to November 2021, accredited cancer programs enrolled in the QI project completed a total of 859 QI projects, which included implementing evidence-based screening interventions at each local program aimed at reducing cancer screening deficits exacerbated by the pandemic.
Each accredited program was encouraged to select one or more target screening areas of greatest importance to their local community: breast, colorectal, lung, or cervical cancer.
The researchers found that most cancer programs (79%) enrolled in the QI project successfully restored screening rates to pre-pandemic volumes and achieved a minimum of 10% growth in screening. They did not find any major differences between hospital characteristics, though there were some variabilities based on the type of cancer screening.
The success of the QI project, the researchers added, can be attributed to the motivation of healthcare professionals to reverse pandemic-related screening deficits, the presence of existing cancer accreditation resources, and the rapid formation of the national-level QI project when it was needed the most.
"Any quality improvement project, even at a local level, is difficult to accomplish and takes a concerted effort," said lead author Rachel Hae-Soo Joung, MD, MS, a PGY-6 general surgery resident at the Northwestern University Feinberg School of Medicine.
"I think this study speaks to the larger implications of how a quality improvement project can be implemented in a swift manner to address urgent needs. With cancer screening, we didn't want to wait for two years to realize that there had been dips in volumes. We wanted data readily available to help us understand and address missed screenings."
More information: Rachel Hae-Soo Joung et al, Evaluation of a National Quality Improvement Collaborative on Improving Cancer Screening, JAMA Network Open (2022). DOI: 10.1001/jamanetworkopen.2022.42354
Rachel H. Joung et al, A national quality improvement study identifying and addressing cancer screening deficits due to the COVID‐19 pandemic, Cancer (2022). DOI: 10.1002/cncr.34157
Journal information: JAMA Network Open , Cancer
Provided by American College of Surgeons





Post comments