
by Cedars-Sinai Medical Center
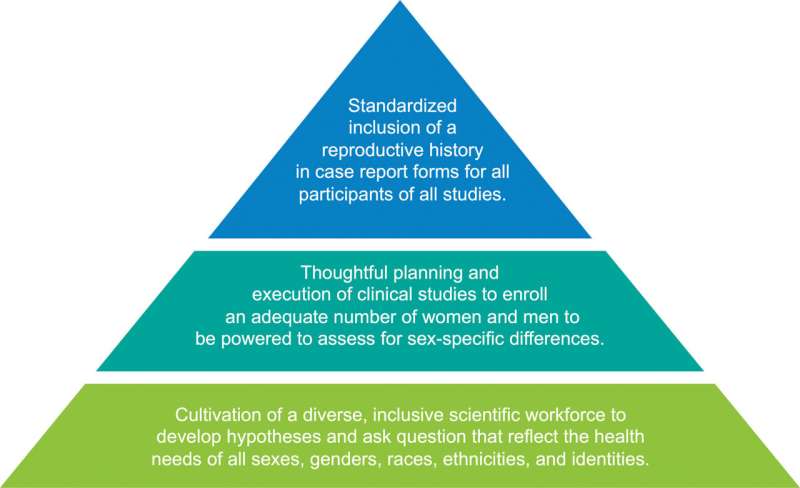
Fundamental changes needed to foster the implementation of inclusive research that addresses gaps in the cardiovascular health of women in the next century. Credit: Circulation Research (2024). DOI: 10.1161/CIRCRESAHA.123.323182
Experts at the Smidt Heart Institute at Cedars-Sinai who have studied progress made over decades of research say there's still a long way to go before medical science fully understands how heart disease is different in women than men.
But there is hope, according to Natalie Bello, MD, MPH, director of Hypertension Research in the Department of Cardiology, and colleague Susan Cheng, MD, MPH, the Erika J. Glazer Chair in Women's Cardiovascular Health and Population Science, who recently authored a perspective article in the journal Circulation Research.
The paper reflects on women's cardiovascular health during the past century and looks ahead to the many advances happening in the field. Bello spoke with the Cedars-Sinai Newsroom to share more.
What do women need to know about their cardiovascular health?
Heart disease is the No. 1 cause of death in women, but surveys show women tend to think they are more likely to die of cancer, particularly breast cancer. The most important thing to remember is that heart disease kills more women than all types of cancer combined.
Are some women at greater risk than others?
Almost 20% of women who get pregnant experience complications, such as high blood pressure, preeclampsia or gestational diabetes, that have important implications for their future heart health. These conditions are associated with a higher incidence of heart disease that often happens early in the lifespan.
What progress has been made?
Thanks to pioneers like C. Noel Bairey Merz, MD, director of the Barbra Streisand Women's Heart Center in the Smidt Heart Institute, the medical community is now actively involved in the advancement of women's heart disease research and care. Her leadership in this area has broadened the visibility of gender differences in things like heart attack symptoms and the diagnosis of small vessel heart disease.
Could you give an example of how increased research into women's cardiovascular health has led to better treatment for women?
There is a now a blood test approved by the U.S. Food and Drug Administration, developed by Cedars-Sinai investigators, that we can use to understand a woman's risk for preeclampsia. It helps tell us when a pregnant woman is safe to go home or if she needs to stay in the hospital for closer monitoring, treatment, or early delivery. We use it very frequently.
This is just one of many examples of how Cedars-Sinai has led to women's heart health.
When should women think about their cardiovascular health?
At age 20, women should establish care with a primary care physician and have their cardiovascular risk assessed. At a minimum, all women should visit a primary care provider annually for a blood pressure check.
What are the best ways to prevent cardiovascular disease?
Learn about your personal risk and ways you can modify the disease. That advice is based on the knowledge that 80% of cardiovascular disease is preventable. By doing things like stopping smoking, eating healthy, maintaining a healthy body weight, exercising, and sleeping well, we can prevent or delay the progression of heart disease.
Why is it that women's cardiovascular health has been ignored?
In a paper published in 1912, a researcher named Dr. James Herrick and colleagues described heart disease as something that occurred in men. But they published another paper in 1928 showing that the same thing was happening in women. For whatever reason, the follow-up work never gained traction, and that set the stage for heart disease being seen as a man's issue.
Early epidemiologic research also demonstrated a delay in the onset of heart disease in women compared with men. Noting that women's risk seemed to increase after menopause, estrogen was believed to be protective, and premenopausal women's risk for heart disease was thought to be low.
We now realize that societal issues and habits at the time also influenced risk: Men were more likely to smoke, and women didn't start smoking socially until later in the last century. Unfortunately, when smoking became socially acceptable for women, there was an uptick in women's heart disease as a result.
I think one of the main reasons women's cardiovascular health wasn't really investigated is that there was not as much diversity in science and medicine at the time. If you don't experience things, you don't know what questions to ask. I'm not saying it's impossible, but a bunch of men sitting around a table aren't necessarily going to ask each other, "I wonder how excessive menstrual bleeding impacts heart disease risk?" and decide to examine that in a research study.
What can women who aren't scientists do to ensure the medical system addresses their needs?
It often takes people outside of the scientific community to remind us that we need to examine certain issues in women's health. A lot of times, it comes from patients who experienced something in their own pregnancy or in their own heart health journey and either started a foundation or lobbied elected officials to increase funding for research related to women.
It's also important for women to feel empowered to discuss their concerns with their clinicians, and if they feel they aren't being listened to, they should find another person to listen to their symptoms and work them up appropriately.
More information: Natalie A. Bello et al, Where Do We Go From Here: Reflections on a Century in Women's Cardiovascular Health Research, 1924–2024, Circulation Research (2024). DOI: 10.1161/CIRCRESAHA.123.323182
Provided by Cedars-Sinai Medical Center







Post comments