
By Anne Asher, CPT
Medically reviewed by Stuart Hershman, MD
Revision spine surgery may be deemed necessary forr a number of reasons. But how do you know if you really need that 2nd back surgery? Check this list to start your research.
1
Recurrent Disc Herniations

Herniated disc diagram. BSIP/UIG/Universal Images Group/Getty Images
If, after a discectomy, you again have sciatica, pain down your arm, or other herniated disc symptoms, you may have a recurrent herniation or cervical radiculopathy. A recurrent disc herniation is herniation of more disc material in the same place as the herniation that initially led to surgery.
A discectomy typically removes only those pieces of disc material (called fragments) that have become partially or fully disengaged from the main disc. You still have your disc, and it is still possible to herniate the part that's left.
Dr. Joshua D. Auerbach, Chief of Spine Surgery at Bronx-Lebanon Hospital Center in New York City, likens a discectomy to eating a piece of cheesecake, especially for those who are passionate about this delicacy.
While you are happily focused on the gustatory experience, he says, chances are bits of cheesecake will separate from the main slice. Some will land on the plate, others may land on the rim of the plate, and still others may fall off completely. In this situation, most people would discard those fragments that fall off the plate, but continue eating the main slice.
The discectomy analogy works similarly: The non-usable pieces are cleared away from the main structure, leaving the rest of your disc, or piece of cake, intact.
2
Pseudoarthrosis
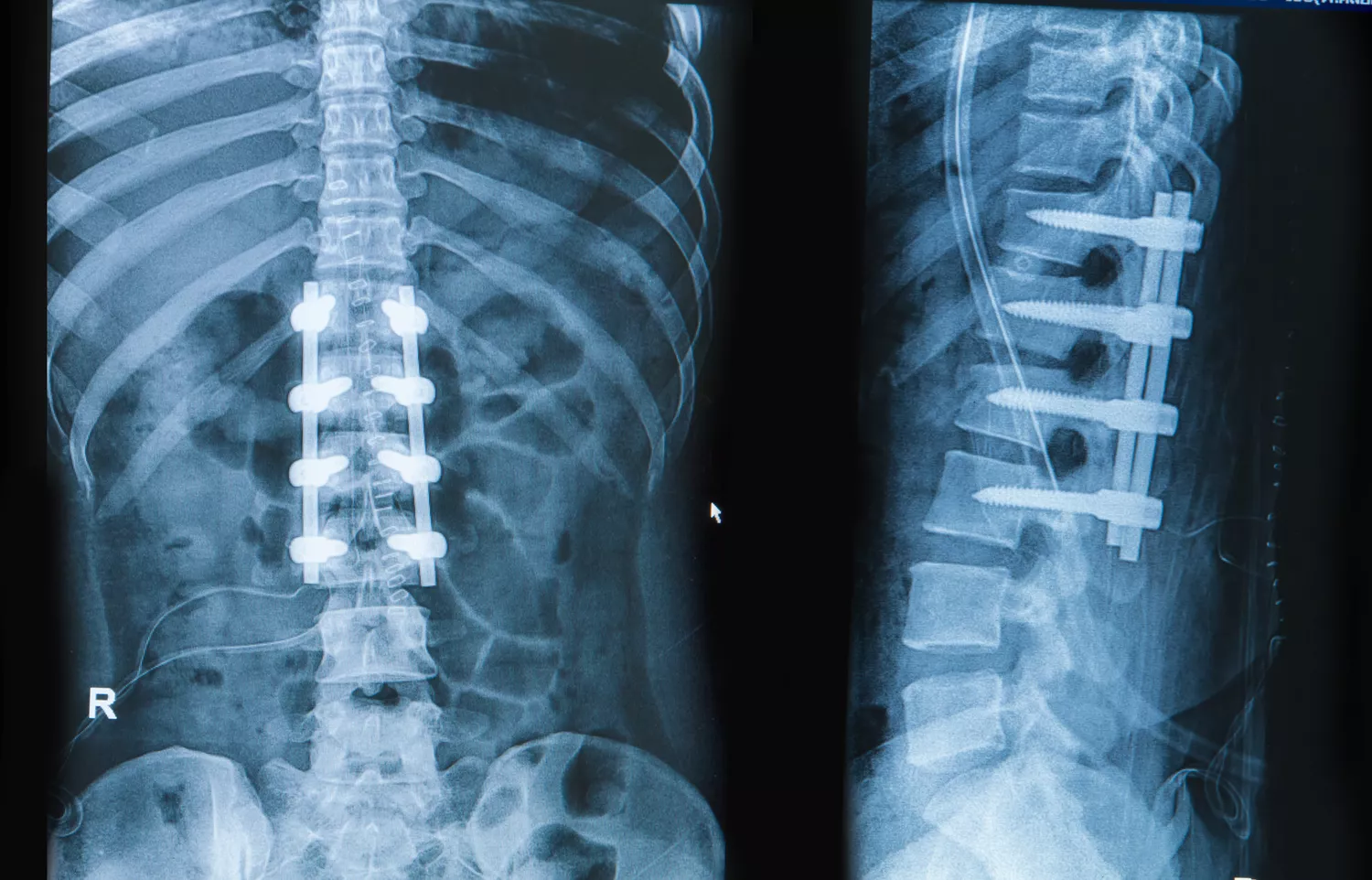
plepraisaeng / Getty Images
Pseudoarthrosis is a term that describes a lack of bone fusion later than one year after a spinal fusion surgery.
Pseudoarthrosis is very common, occurring in up to 68% of lumbar fusions, according to Auerbach. Of these, between 6 and 36% require a re-operation, he says.
Some things that may play a role in the development of pseudoarthrosis after your first surgery include:
The nature of your original diagnosis
Type of hardware (or lack thereof) installed
Type of bone graft, if any, used
Your health habits and condition. For example, if you smoke or take corticosteroids, your risk for pseudoarthrosis may be increased.
If you have a spinal fusion in which no plates, screws or other hardware are installed.
In his chapter on revision lumbar spine surgery for the medical text entitled The Textbook of Spinal Surgery, 3rd Edition, Auerbach cites studies that show fusions performed without the implantation of hardware may increase your risk for pseudoarthrosis by 70%. That number is much lower -- 10% -- for spinal fusions in which hardware is placed, he reports.
3
Adjacent Segment Disease
SEBASTIAN KAULITZK / Collection: Science Photo Library / Getty Images
ASD, or adjacent segment degeneration, is a condition in which anatomical changes occur at spinal joints above and/or below the place a back surgery is done.
Auerbach says that when ASD occurs, it generally does so after about two or more pain-free years.
Experts don’t fully know if it is the back surgery or the natural progression of degenerative changes in the spine that’s responsible for ASD.
Frank Cammisa, Jr., M.D., Chief of the Spine Service at the Hospital for Special Surgery in New York, says factors other than the surgical procedure may be at work in the development of the degenerative changes we call ASD. "Many times, ASD is blamed on the fact that a patient has a fusion; however, even if the patient never underwent a fusion they may still develop degenerative changes at another level."
A study done by Song, et. al, entitled, "Adjacent segment degenerative disease: is it due to disease progression or a fusion-associated phenomenon? Comparison between segments adjacent to the fused and non-fused segments," published in the November 2011 issue of European Spine Journal found that "adjacent segment disease is more a result of the natural history of cervical spondylosis than the presence of fusion."
Auerbach says that biomechanical studies do show extra stress at adjacent levels following a fusion. Because fusion tends to increase the steepness of the angle between the two bones of an intervertebral joint, the way your spine moves will likely be altered. This may impose extra pressure on some areas of the joint.
“The discs pick up the slack,” he tells me.
According to Auerbach and others, this type of increased stress is a big reason why many in the industry are pushing for the development of motion preservation surgical techniques and devices. Advances in technology -- for example, total disc replacements -- enable healthcare providers to treat the problem without sacrificing movement in the affected area.
In case you are wondering, there are studies that show an advantage to having a cervical disc replacement over a spinal fusion, although not all the questions have been answered (as of 2016). For example, in an analysis of three studies comparing the results of cervical disc replacements with spinal fusion two years after the procedure, researchers found that people who had arthroplasty (disc replacement) were 44% less likely to need a second surgery. That same study did not report on any significant benefit of arthroplasty for minimizing or avoiding ASD, however.
4
Revision TDR

BSIP / UIG / Collection:Universal Images Group / Getty Images
Total disc replacement, often called TDR for short, is a relatively new surgery (in the United States, at least) that is seen by some spine experts as a viable alternative to spinal fusion surgery. Disc replacements have been done in Europe for a while, but the U.S. is adopting this technology more slowly.
Auerbach says that only about 0-5% of patients referred for spine surgery fit the criteria for a safe and successful total disc replacement procedure. If you are not a candidate, but you have one anyway, he says, you may experience complications.
One of the most common complications leading to a revision TDR (as a second disc replacement surgery is sometimes called) is device failure. Examples of device failure include malfunctioning of the prosthetic disc implanted in your spine, or when the device shifts its position (extrudes).
Cammisa adds that because a disc replacement preserves motion, normal degenerative changes can occur at the facet joints. If this degeneration becomes too painful, he says, your healthcare provider may suggest a spinal fusion as your revision surgery.
5
Problems With Implanted Hardware
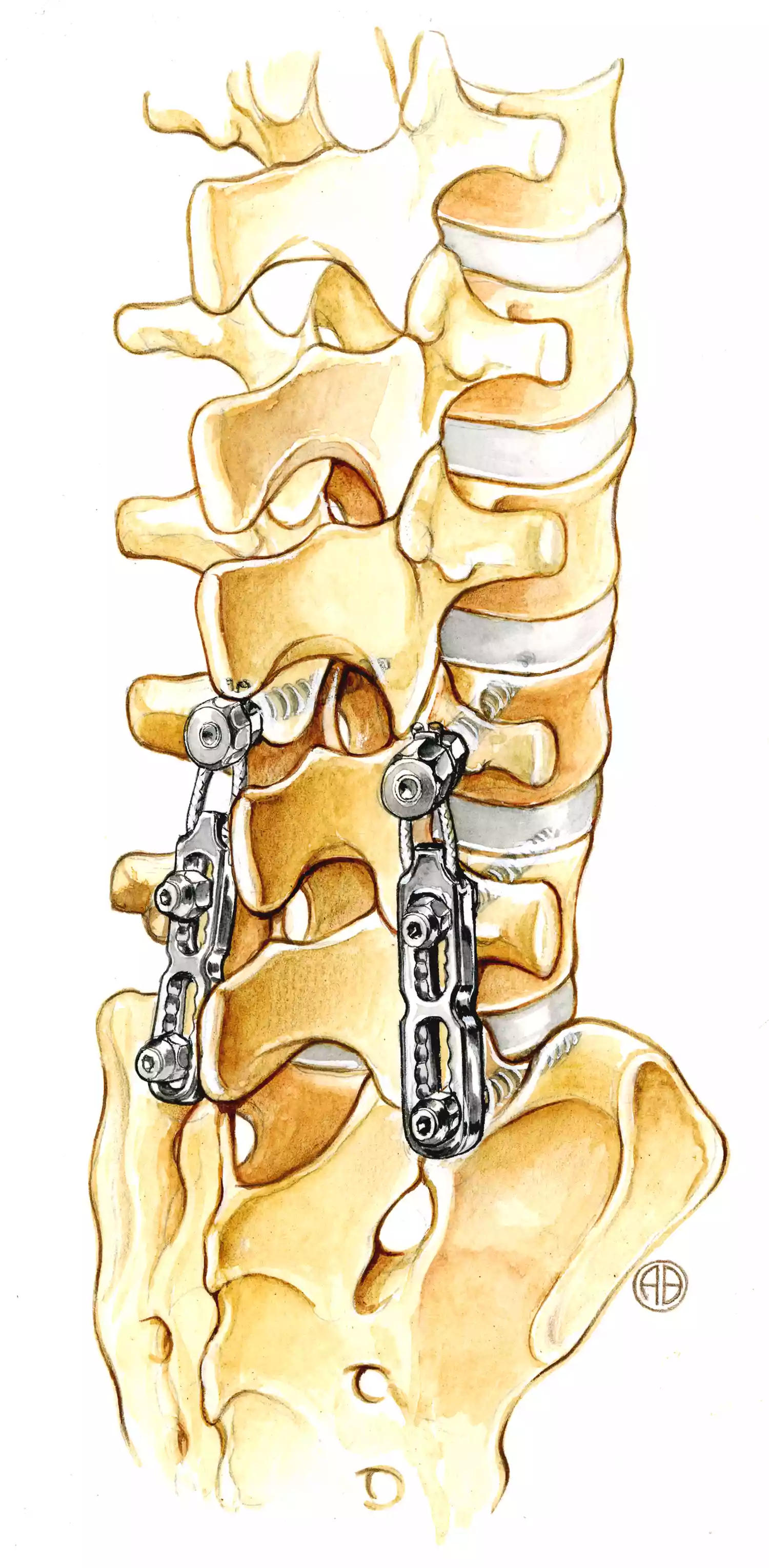
BSIP / UIG / Collection: Universal Images Group / Getty Images
More rarely, you may run into problems with the hardware that was implanted in your spine. This includes prosthetic discs, as mentioned above, as well as hardware used for spinal fusion and other types of back surgery. The instrumentation, as it is sometimes called, may break, or the surgeon may have placed it in the wrong position during the procedure.
One type of hardware problem resulting from a back surgery is a syndrome known as “painful hardware." In this case, the implanted items are simply too uncomfortable, Auerbach says. "This typically occurs when they can be easily felt through the skin."
Camissa says that pain due to painful hardware syndrome usually arises from soft tissue (i.e. your muscles, ligaments, tendons, and fascia).
Addressing painful hardware syndrome sometimes requires surgery to remove the offending items. Cammisa informs me that revision surgery for painful hardware syndrome is usually due to the placement of the hardware, not the device itself. "It is extremely uncommon to have to remove instrumentation because of pain that's caused by the device," Cammisa confirms.
Revision surgery for painful hardware is usually done immediately.
Sources
Benglis D, Wang MY, Levi AD. A comprehensive review of the safety profile of bone morphogenetic protein in spine surgery. Neurosurgery. 2008;62(5Suppl2):ONS423-31. doi:10.1227/01.neu.0000326030.24220.d8
Etminan M, Girardi FP, Khan SN, Cammisa FP Jr. Revision strategies for lumbar pseudarthrosis. Orthop Clin North Am. 2002;33:381–392. doi:10.1016/s0030-5898(02)00005-6
Patel A, Spiker W. Update on the diagnosis and treatment of lumbar nonunions. Semin Spine Surg. 2008;20(1):20-26. doi:10.1053/j.semss.2007.11.004
Song KJ, Choi BW, Jeon TS, Lee KB, Chang H. Adjacent segment degenerative disease: is it due to disease progression or a fusion-associated phenomenon? Comparison between segments adjacent to the fused and non-fused segments. Eur Spine J. 2011;20(11):1940–1945. doi:10.1007/s00586-011-1864-9
Upadhyaya C, Wu J, Balamurali G et al. Combined results of the 3 US IDE randomized cervical arthroplasty trials with 2-years of follow-up. Neurosurgery. 2010;67(2):543-543. doi:10.1227/01.neu.0000386995.74131.4b
Auerbach, J., MD. Chief of Spine Surgery, Bronx-Lebanon Hospital Center, Assistant Professor of Surgery, Albert Einstein College of Medicine. Phone Interview. March 2012.
Auerbach JD, Kuklo TR. Revision Lumbar Spine Surgery. In: Bridwell KH, DeWald R, eds. The Textbook of Spinal Surgery, 3rd Edition. Philadelphi., Lippincott 2011.
Cammisa, F., MD, Chief of the Spine Service at Hospital for Special Surgery. New York. Email Interview. March 2012.
By Anne Asher, CPT
Anne Asher, ACE-certified personal trainer, health coach, and orthopedic exercise specialist, is a back and neck pain expert.






Post comments