
by H. Lee Moffitt Cancer Center & Research Institute
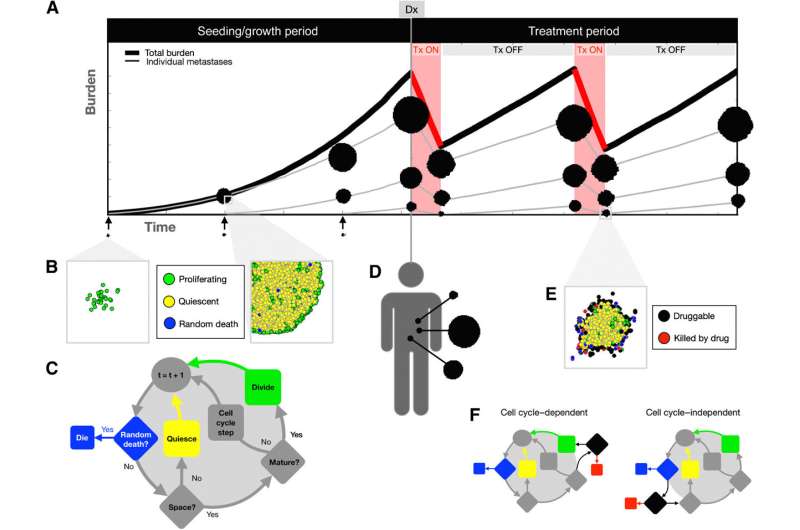
Mathematical model overview and design. A, Simulated treatment trajectory. During the seeding/growth phase, metastases are seeded and grown until reaching a specific total burden at diagnosis (Dx). The treatment period follows, during which, therapy is applied until the tumor burden reaches half of the original value, and therapy is withdrawn until the tumor burden reaches the original value again, where the treatment cycle begins anew. B, For each metastasis, individual cells are seeded in a separate off-lattice domain. Total burden used for treatment decisions is defined as the sum of all cells in the whole system of metastases. C, ABM decision flowchart for each individual cell over a time step. D, After reaching the designated burden, the treatment period begins. E, Cells are considered druggable if they lie near the outside edge of the mass (see Supplementary Methods for details), and they can only be killed by the drug if they are druggable. F, Metastases are either subjected to a cell cycle–dependent or cell cycle–independent drug, acting at the point in the decision flowchart shown. Credit: Cancer Research (2023). DOI: 10.1158/0008-5472.CAN-22-2558
Most cancer deaths are due to the metastatic spread and growth of tumor cells at distant sites. Identifying appropriate treatments for patients with metastatic disease is challenging because of limited biomarkers and detection capabilities, and poor characterization of metastatic tumors.
In a new study published in Cancer Research, Moffitt Cancer Center researchers demonstrate how mathematical modeling combined with dynamic biomarkers can be used to characterize metastatic disease and identify appropriate therapeutic approaches to improve patient outcomes.
Metastatic tumors can vary in size, location and composition. Metastases also vary within an individual patient, making treatment decisions challenging. Physicians use biomarkers collected from blood specimens, tissue biopsies and images to identify appropriate treatment strategies.
However, these techniques are limited by single timepoints, poor resolution of smaller lesions and an inability to provide information on individual metastases. Scientists are investigating the potential of dynamic biomarkers to overcome the limitations of standard biomarker approaches.
"Dynamic markers base prognosis not on the absolute value of measurement at a single time point, but on the relative change over time. For example, PSA doubling time may stratify patients with prostate cancer who are likely to respond better to chemotherapy, progress to metastatic disease or die from the disease," said Jill Gallaher, Ph.D., a research scientist in the Department of Integrated Mathematical Oncology at Moffitt.
Moffitt researchers used mathematical modeling and dynamic biomarkers to identify the characteristics of metastatic disease that are associated with better patient outcomes to treatment. They focused their analysis on a biomarker called prostate-specific antigen (PSA) that is commonly used in the diagnosis and treatment of patients with prostate cancer.
The researchers performed their study with data from 16 patients treated in a clinical trial of adaptive therapy. During adaptive therapy, patients are given breaks from treatment based on their change in PSA levels. This approach is designed to prevent the development and growth of drug resistant tumors that cause treatment failure.
The researchers assessed dynamic PSA biomarkers during the first cycle of adaptive therapy, which includes the time it takes to reduce the PSA burden by 50% when treatment is on and the time it takes to regrow to the original value when the treatment is off.
They identified several key relationships between metastatic disease and the biomarkers, including metastases that were larger in size had longer treatment cycles; metastases with a higher proportion of drug-resistant cells slowed the cycle; and metastases that had a faster cell turnover rate had a faster drug response time and a slower time to regrow.
They also relate PSA dynamics to clinical variables, including Gleason score, a grading system used to show how abnormal the prostate cancer cells look and how likely the cancer will advance; the change in the number of metastases during a cycle; and the total number of cycles over the course of treatment.
The team performed additional modeling to compare adaptive therapy to continuous therapy during which no treatment breaks are given. They discovered that differences between metastatic tumor compositions favored continuous treatment, and differences within metastatic tumor compositions favored adaptive schedules.
These observations suggest that it may be possible to use mathematical modeling approaches combined with dynamic and standard biomarkers to improve the characterization of patients' disease and help identify appropriate treatment options.
"Multiscale mathematical models, such as the one proposed here, can help disentangle the multidimensional nature of cancer and lead to a better understanding of the drivers of treatment success and failure. While this work is only a first step, it shows that model-informed analysis of biomarkers and visible metastases during a single cycle of adaptive therapy may be useful in identifying important features of the metastatic population to provide further support for treatment decision-making," explained Alexander Anderson, Ph.D., chair of the Department of Integrated Mathematical Oncology at Moffitt.
More information: Jill Gallaher et al, Intermetastatic and Intrametastatic Heterogeneity Shapes Adaptive Therapy Cycling Dynamics, Cancer Research (2023). DOI: 10.1158/0008-5472.CAN-22-2558
Journal information: Cancer Research
Provided by H. Lee Moffitt Cancer Center & Research Institute







Post comments