
by American Heart Association
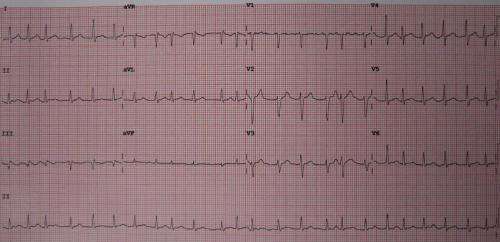
A 12 lead ECG showing atrial fibrillation at approximately 150 beats per minute. Credit: James Heilman, MD/Wikipedia/CC BY-SA 3.0
Treatment with the Type 2 diabetes medication metformin, lifestyle changes, or a combination of both did not improve atrial fibrillation (AFib) burden or progression when compared with standard care, according to preliminary late-breaking science presented Nov. 18 at the American Heart Association's Scientific Sessions 2024. The meeting, held Nov. 16–18, 2024, in Chicago, is a premier global exchange of the latest scientific advancements, research and evidence-based clinical practice updates in cardiovascular science.
Metformin is a common medication to treat Type 2 diabetes because it decreases the amount of glucose made in the liver, which helps control blood sugar levels. AFib is the most common form of arrhythmia, an abnormal heart rhythm, and it can lead to stroke, heart failure or other cardiovascular complications. More than 12 million people are projected to have AFib in the U.S. by 2030, according to the American Heart Association's 2024 Heart Disease and Stroke Statistics.
Previous research has indicated that lifestyle/risk factor modification to reduce cardiovascular risk factors can help reduce AFib burden, a quantitative term used to refer to the amount of time a person's heart is experiencing the abnormal rhythms of AFib. Additionally, the study authors noted that recent genomic and genetic studies have suggested that improving the biochemical levers handling metabolic stress—the response to stressors that can cause an imbalance in energy supplies to cells—might help AFib.
"Interventions including weight loss, exercise and metformin act on an enzyme called AMP kinase, which is the master regulator of metabolic stress in the cells," said lead study author Mina K. Chung, M.D., FAHA, a cardiologist and professor of medicine at the Cleveland Clinic in Ohio. "In this study, we examined whether interventions including these might reduce AFib burden or progression."
In this trial, called TRIM-AF, 149 adults who had AFib were randomly assigned to one of four treatment groups: standard of care (participants received educational pamphlets on healthy diet and exercise without individual counseling); metformin only; a lifestyle/risk factor modification program (including referral to a preventive cardiology team for diet and nutrition counseling as well as for an exercise prescription and to address other cardiovascular risk factors); or both metformin and the lifestyle/risk factor modification program.
The patients in the lifestyle/risk factor modification groups were offered a diet and exercise visit every three months in the first year of the study and every six months in the second year.
The metformin-only group, the lifestyle/risk factor modification group and the combination lifestyle/risk factor modification and metformin group—but not the standard of care group—lost weight by the one-year follow-up but did not meet activity or fitness targets.
The study was open label, meaning both the researchers and participants knew which groups participants were in and which interventions they were receiving. Participants enrolled in the study had AFib and an implanted cardiac device, such as a pacemaker or implantable cardiac defibrillator, which could record the daily AFib burden, or average percentage of time each day they spent experiencing arrhythmia. Participants were followed for up to two years after enrollment in one of the four groups.
After the one-year follow-up, the analysis found:
The AFib burden decreased over time in the standard of care group, the lifestyle/risk factor modification group, and the lifestyle/risk factor modification and metformin group. The metformin group initially tended to show worsened AFib burden compared to standard of care, but at later time periods was not significantly different from baseline or standard of care, the researchers noted.
There were no significant differences in AFib burden change between the four groups.
The median baseline AFib burden was 5.5% in the standard of care group, 1.8% in the metformin group, 2.1% in the lifestyle/risk factor modification group and 6.5% in the combined lifestyle/risk factor and metformin group.
At 9–12 months, median AFib burden was 0.67% (relative change -73.5%) in the standard of care group, 0.62% (relative change -48.9%) in the metformin group, 0.13% (relative change -85.9%) in the lifestyle/risk factor modification group and 0.90% (relative change -72.4%) in the combined lifestyle/risk factor modification and metformin group, the researchers noted.
More than one-third of the study's participants, in the two metformin groups, either did not start or had to stop the medication due to gastrointestinal side effects, which include diarrhea, nausea and stomach discomfort, the researchers noted.
All three intervention groups experienced weight loss (an average of 2.4% of their starting body weight in the metformin group, 2.1% in the lifestyle/risk factor modification group and 4.4% in the combined lifestyle/risk factor modification and metformin group), while the standard care group did not significantly change (lost 0.5%).
Neither of the lifestyle modification groups—those taking metformin and those not taking it—achieved the target weight-loss goal, an average of 10% of participant's starting body weight, and fitness targets (2 MET improvement on stress testing) set for the study. Device-recorded physical activity times did not increase, and fitness, assessed through exercise testing, showed no significant improvement.
However, the researchers did see an improvement in atrial fibrillation symptom scores in the two lifestyle modification groups. According to Chung, this reinforces how exercise and weight loss may help people feel better.
"We were especially surprised by the decrease in AFib burden in the standard of care group. We analyzed periods before randomization and saw in all groups that the AFib burden increased. Then, upon randomization, we saw a decrease in AFib burden in all groups," said Chung, who was also vice chair of the joint American Heart Association/American College of Cardiology 2023 Guideline for the Diagnosis and Management of Atrial Fibrillation.
"It is possible that the written [Cleveland Clinic] literature on diet and exercise we distributed to the standard of care group for participation in the study could have had a greater effect on reduction of AFib burden than we thought. This was a group of patients who were motivated with discussions to join a lifestyle/risk factor modification study.
"I think one of the key messages from this study is that talking to patients with AFib about lifestyle/risk factor modification and giving them written instructions or more intensive individualized instructions performed well.
"The metformin group also experienced a notably high rate of intolerance, which could have increased stress, and we do not know yet whether those who tolerated the metformin had other improvements," Chung said.
"However, at this time, metformin alone should not be recommended as an upstream therapy for atrial fibrillation. The combination of metformin and lifestyle/risk factor modification appeared to show some benefits, but these only reached levels similar to the standard of care arm."
The researchers said they will continue to analyze the data to determine if people who tolerated metformin and stayed on it for two years have a reduction in AFib burden. They will also examine AFib burden changes in people who had a higher AFib burden when they enrolled in the study.
One message from this research is the importance of randomized studies that compare interventions. "Prior nonrandomized studies have suggested a benefit of metformin in reducing AFib, however, non-randomization may have introduced bias," Chung said.
The TRIM-AF study had several limitations, including its small size. In addition, the COVID-19 pandemic began in the middle of the study, which made it difficult to recruit participants and conduct in-person visits. Chung noted that they adapted by changing the protocol to allow virtual visits and by reducing the sample size from 200 to 150 participants. The study will complete two-year follow-up in the fall of 2025.
Study details, background and design
The ongoing, two-year follow-up study, which started in 2018, is being conducted at the Cleveland Clinic in Ohio.
The study population included 149 adults who had AFib at the time of enrollment. Adults were evenly randomized into four treatment groups: 37 in the metformin only group; 35 in the lifestyle/risk modification group; 38 in the combined metformin and lifestyle/risk modification group; and 39 in the standard of care group.
At study enrollment, 118 (79.2%) participants had a diagnosis of hypertension; 13 (8.7%) had a diagnosis of Type 2 diabetes; 57 (38.3%) had a diagnosis of coronary artery disease; 102 (68.5%) had a pacemaker; and 47 (31.5%) had an implantable cardioverter defibrillator. There were no significant differences in the baseline characteristics between the groups, except there were more patients with hypertension in the two groups not receiving metformin compared to the two groups that received metformin (86.5% and 72%, respectively).
Study participants had an average age of 74. 61% of participants self-identified as men; 39% as women. 96.6% of the participants identified as white adults, 2.7% as Black adults and 0.7% as Asian adults.
Provided by American Heart Association






Post comments