
Everything You Need to Know About Stomach Pain
By Barbara Bolen, PhD
Medically reviewed by Robert Burakoff, MD
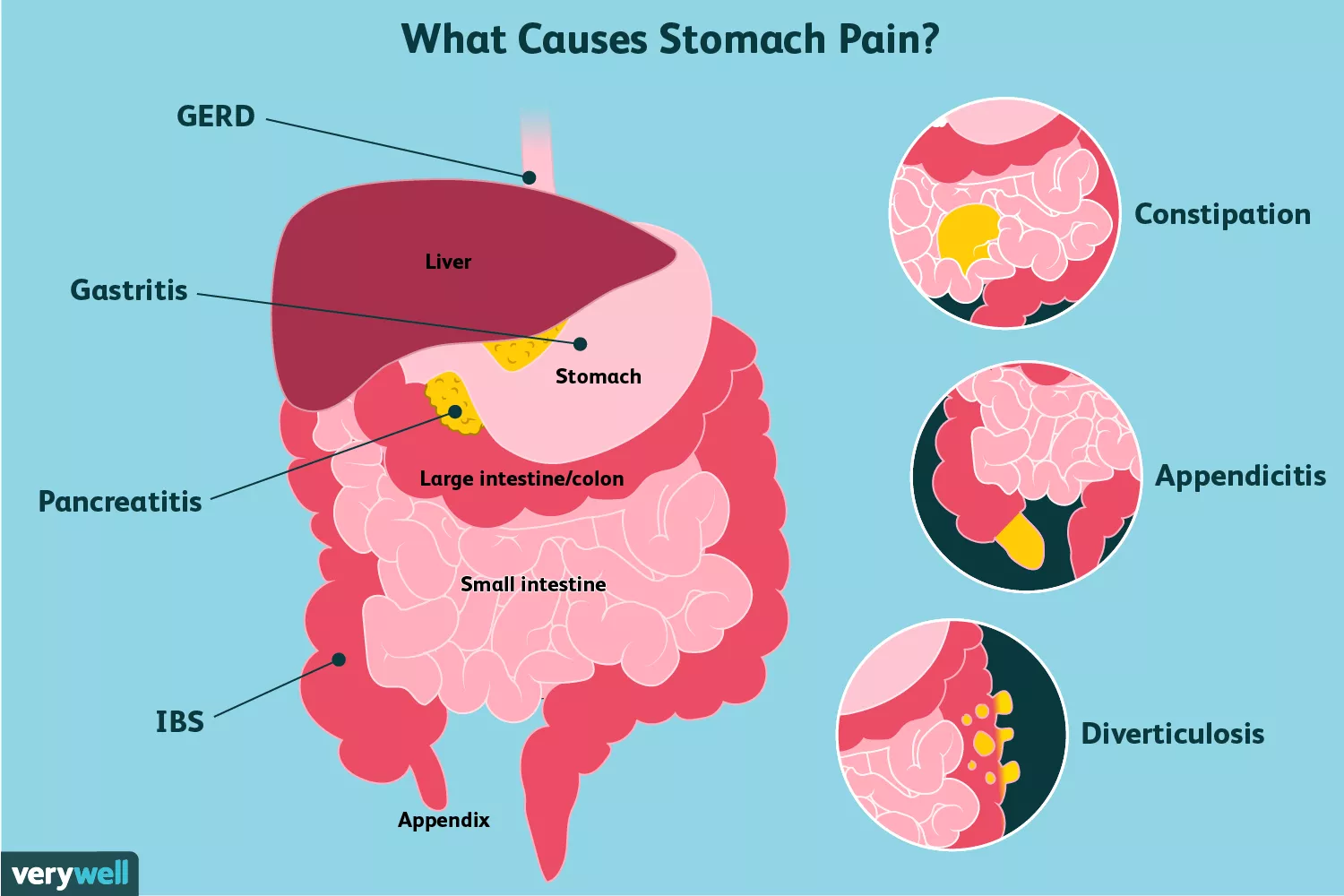
Stomach pain is often caused by something you ate, an infection, or a gastrointestinal condition. Depending on the cause, stomach pain may also be accompanied by other gastrointestinal symptoms, such as nausea, bloating, gas, or indigestion.
At-home treatments and lifestyle modifications can sometimes be enough to ease your stomach pain. If they aren't, or if symptoms are severe, persistent, or worsening, you need to see a healthcare provider to investigate the cause.
This article covers several possible causes of stomach pain. It also explains how those conditions may be treated, along with when to see a healthcare provider.
Understanding Stomach Pain
The stomach, of course, is its own unique organ. But when people use the term "stomach pain," many mean pain related to the gastrointestinal tract. As such, we also do so here.
Typically speaking, perceived stomach pain that occurs in the part of the abdomen nearer to the ribs involves the upper gastrointestinal (GI) tract, which includes the esophagus, stomach, and small intestines.1
Pain occurring in the lower abdomen tends to be related to the lower GI tract, which is comprised of the large intestine (colon), rectum, and anus.2
When you are experiencing stomach pain, it can be hard to pinpoint exactly where the pain is located. If you have any concerns about what you are feeling, don't hesitate to reach out to a healthcare provider.
Upper Gastrointestinal Tract
Besides the stomach bug or the occasional bout of indigestion, here are some health conditions that cause more persistent stomach pain in the upper gastrointestinal tract:
Peptic Ulcer
Peptic ulcer is an open sore in the stomach or duodenum (the first part of the small intestine).
Peptic ulcer pain is typically felt in the upper mid-abdomen. It may occur at night and wake you up. It may also occur about one to three hours after a meal, or when you have an empty stomach.3
Other possible symptoms of peptic ulcer disease include:
A feeling of fullness
Problems drinking as much fluid as usual
Nausea and vomiting
Bloody or dark, tarry stools
Chest pain
Fatigue
Vomiting, possibly bloody
Weight loss
Ongoing heartburn
Most peptic ulcers are caused by either the bacterium Helicobacter pylori or the use of nonsteroidal anti-inflammatory drugs, which may irritate and alter the protective mucosal layer of the digestive tract.4
Anytime you have blood in your stool or vomit, you need to get medical attention immediately. Bloody stool or vomit can be a sign of a life-threatening medical condition.3
Gastritis
Gastritis is the medical term for inflammation in the lining of the stomach. Gastritis can be caused by many things, such as:5
Drinking too much alcohol
Smoking
Extreme stress
Long-term use of aspirin and over-the-counter pain medications
Infections caused by bacteria and viruses
Major surgery
Traumatic injury and burns
In some cases, the condition will be idiopathic (meaning no cause is ever found).
Gastritis pain is typically felt in the upper part of the abdomen or belly. There may be other symptoms, too, such as:5
Loss of appetite
Nausea and vomiting
Blood in stools or vomit
Again, if you vomit blood or notice it in your stools, do not wait to see a healthcare provider.
Gastroparesis
Gastroparesis, also called delayed gastric emptying, is a condition in which the stomach is slow to empty its contents into the small intestine. This condition is common in people with diabetes, but may also occur idiopathically (without an identified cause).6
Besides aching or cramping pain in the upper abdomen, other symptoms of gastroparesis include:7
Feeling full long after eating a meal
Nausea or vomiting
Excessive bloating
Excessive belching
Heartburn
Poor appetite
Some medications can worsen gastroparesis symptoms, such as:7
Narcotic pain medications, like codeine
Some antidepressants, like amitriptyline
Some anticholinergics (medicines that block certain nerve signals)
Some medicines used to treat overactive bladder
Pramlintide, a blood pressure-lowering medication
Gastroesophageal Reflux Disease
Gastroesophageal reflux disease (GERD), a more serious form of acid reflux, is a condition in which stomach acid leaks back into the esophagus, causing a burning sensation in the chest or throat.
GERD pain may be felt in the upper abdomen or chest. Some other symptoms of GERD include:8
Regurgitation
Trouble swallowing
Heartburn
Hoarseness
Cough
A feeling like there is a lump in the throat
Chest pain can sometimes be a sign of heart attack or another life-threatening medical emergency. Get medical attention immediately if you are experiencing new or unusual chest pain.
Esophagitis
Your esophagus is the tube that carries food from your mouth to your stomach. Esophagitis refers to irritation and inflammation of the lining of the esophagus, which may occur for many reasons, including:9
GERD
Chronic vomiting
Some anti-inflammatory medications like aspirin
Some medical procedures, like radiation therapy
Infections that weaken the immune system
Allergies, especially food allergies
Esophagitis pain is felt behind the breastbone and is sometimes described as a burning, heavy, or sharp sensation that may be constant or come and go. The pain may also be worse after meals or when you lie flat.10
Left untreated, esophagitis can progress to a condition called Barrett's esophagus. This condition may increase your risk for esophageal cancer.
Gallstones
Gallstones are caused by the crystallization of bile in the gallbladder. Gallstones often do not cause symptoms at first. Symptoms usually begin when gallstones grow larger, or when they start to obstruct the bile ducts (a condition called acute cholecystitis).
Gallstone "attacks" commonly occur at night or after a fatty meal. The pain is felt in the upper abdomen which increases rapidly and may persist from 30 minutes to several hours.
Other symptoms of gallstones include:11
Pain in the back between the shoulder blades
Pain in the right shoulder
Nausea or vomiting
Fever and chills
Jaundice (yellowing of the skin and eyes)
Abdominal bloating
Intolerance of fatty foods
Belching or gas
Indigestion
The symptoms of gallstones can resemble other life-threatening medical conditions, like heart attack or appendicitis. Know the signs of these conditions, and get help right away if you suspect one is occurring or are not sure.
Pancreatitis
Pancreatitis refers to inflammation of the pancreas, a small gland that releases insulin to regulate your blood sugar levels and also aids in the digestion of fat. Pancreatitis can be acute (sudden) or chronic (long-term).
Alcohol abuse and gallstone disease are the two most common causes of pancreatitis.12
Most people with acute pancreatitis develop severe, constant pain in the upper belly.13 The pain may spread to the back or chest, and it may feel worse after you eat.
Other possible symptoms of pancreatitis include:12
Nausea or vomiting
Rapid heart rate
Fever
Swelling and tenderness in the upper belly
Fluid buildup in the belly
Lowered blood pressure
Jaundice
Celiac Disease
Celiac disease is an autoimmune disorder in which the consumption of gluten causes the immune system to attack the small intestine.14
Celiac pain varies. It can manifest as:
Recurring stomach pain
Muscle cramps or bone pain
Joint pain
Painful, itchy rash
Other possible symptoms of celiac disease include:15
Constant diarrhea or constipation
Weight loss
Gas
Pale, foul-smelling stool
Anemia
Tingling and numbness in the legs
Missed menstrual periods (due to too much weight loss)
Infertility
Early osteoporosis
Teeth changing color
Lactose Intolerance
Lactose intolerance is a condition in which a person lacks the enzyme needed to digest the sugars found in dairy products. People with lactose intolerance typically experience stomach pain, diarrhea, gas, or bloating soon after eating foods like milk or cheese.16
Lower Gastrointestinal Tract
Here are some of the more common health conditions that arise within the colon and rectum.
Constipation
Constipation is very common and often associated with uncomfortable or even painful abdominal bloating from excess gas. Some people with constipation also have:
Very hard or small stools
Increased straining
A feeling that their bowels do not completely empty
Some of the most common causes of constipation include:17
Medications
Lack of exercise
Not drinking enough liquids
Not eating enough fiber
Abuse of laxatives
Diverticulosis
Diverticulosis refers to the development of little pouches within the lining of the colon. The exact cause of diverticulosis is unclear, although it is widely believed to be caused by a lack of adequate fiber in the diet.18
Most people with diverticulosis have no symptoms. Those who do may experience pain and cramps in the stomach, especially in the lower left abdomen.
Infection and inflammation (called diverticulitis) may lead to symptoms ranging from lower abdominal tenderness to severe pain, fever, nausea, and vomiting.19
Appendicitis
The most common symptom of appendicitis is abdominal pain, which usually begins as a dull ache around the belly button.20 Over time, the pain moves to the lower-right part of the abdomen and becomes sharp.
Other associated symptoms include:
Pain that worsens when coughing or walking
Loss of appetite
Nausea or vomiting
Fever
Both GI Tracts
Some health conditions that cause perceived stomach pain may affect both the upper and lower digestive system.
Inflammatory Bowel Disease
Inflammatory bowel disease (IBD), which includes Crohn's disease and ulcerative colitis, manifests with a wide range of gastrointestinal and non-gastrointestinal symptoms.
The hallmark symptoms of Crohn's disease include crampy abdominal pain along with non-blood diarrhea, while the cardinal symptoms of ulcerative colitis include colicky abdominal pain and bloody diarrhea.21
Keep in mind that, while Crohn's disease may affect the entire GI tract from mouth to anus, ulcerative colitis only affects the lower GI tract (colon and rectum).
Irritable Bowel Syndrome
Irritable bowel syndrome (IBS) is characterized by a cluster of symptoms, including:13
Crampy stomach pain
Constipation or diarrhea
The feeling that you haven't finished a bowel movement
Whiteish mucus in stool
IBS symptoms tend to come and go. Although it can be a painful condition, it is not known to damage your digestive tract or lead to other health problems.
Abdominal Hernia
An abdominal hernia, which may cause stomach pain and a visible bulge, occurs when fatty tissue or an organ pokes through a weak or torn area within the abdominal wall.
There are different types of abdominal hernias; for example, an umbilical hernia occurs around the belly button, while an epigastric hernia occurs above the belly button. In men, inguinal hernias (near the groin) are the most common.
Other symptoms of an abdominal hernia include:22
Constipation
Narrow or thin stool
Nausea or vomiting
Fever
Rapid heart rate
Pain around the bulge
Cancer
While less common, upper and lower abdominal pain may be a sign of cancer, including cancer of the:
Ovaries
Pancreas
Stomach
Colon
Liver
Be sure to see your healthcare provider if your pain is persistent or you are experiencing other unusual symptoms like a change in bowel habits, blood in your stool or urine, excessive fatigue, or unexplained weight loss.
When to See a Healthcare Provider
If you ever have sudden and severe stomach pain, seek immediate medical treatment.23 Other symptoms that warrant getting medical attention right away include:
Chest pain
Vomiting up blood or dark-colored flecks
Having black, maroon, or bloody stools
Severe and/or persistent constipation
New-onset pain or swelling around an abdominal hernia site
Dizziness and/or feeling faint
Inability to keep down food or fluids
Diagnosis
After asking about your medical history, your healthcare provider will likely perform a physical examination. The provider may listen to your abdomen with a stethoscope, and press on different areas of your abdomen to evaluate for tenderness, swelling, rigidity, or masses.
If your provider suspects a run-of-the-mill stomach bug, constipation, or another mild condition, they may recommend an over-the-counter medication or a simple lifestyle change.
If your provider suspects a more serious issue is at play, or if they need more information to get to the bottom of your pain, they will likely order further diagnostic tests.24 Tests a provider may order include:
Blood Tests
Depending on your suspected condition, your healthcare provider may order one of many blood tests.
For example, if your healthcare provider suspects gallstones, you will undergo a liver function and bilirubin blood test.
Other blood tests that may be ordered include:
An antibody blood test called IgA tissue transglutaminase for suspected celiac disease
Complete blood count and inflammatory markers, like C-reactive protein (CRP) for suspected inflammatory bowel disease
Pancreatic enzymes (amylase and lipase) for suspected pancreatitis
For a diagnosis of peptic ulcer disease, your healthcare provider will test you for H. pylori infection. You may be tested for H. pylori through an endoscopic biopsy of the stomach (performed during upper endoscopy), a urea breath test, or a stool H. pylori antigen test.
Imaging
Several imaging tests may be used to evaluate the cause of your stomach pain, including an abdominal ultrasound and a computed tomography (CT) scan.24 Two other tests you may not be as familiar with include a barium swallow test and an upper endoscopy.
Barium Swallow
The barium swallow test is an X-ray imaging test sometimes used to evaluate disorders of swallowing, stomach ulcers, and hiatal hernia.25 During this test, a person drinks a thick liquid called barium while X-rays are taken, allowing the esophagus and stomach to be visualized clearly.
Upper Endoscopy
In order to confirm a suspected or potential diagnosis, your healthcare provider may refer you to a gastroenterologist (a healthcare provider who specializes in treating diseases of the digestive tract) for an upper endoscopy.
During an upper endoscopy, while you are sedated, a gastroenterologist inserts a long tube with a camera attached to it into your mouth and down through your esophagus into your stomach.26 During this test, your healthcare provider visualizes the inside of your upper digestive tract and looks for abnormalities. The provider can also use surgical tools passed through the tube to take a biopsy (tissue samples).
Differential Diagnoses
It's possible to have what you think of as stomach pain that doesn't stem from the GI tract at all, but rather from another system.
For example, stomach pain can be easily confused with chest pain. In the event of unexplained chest pain or stomach pain without other classic gastrointestinal symptoms, heart disease needs to be considered. In this case, an electrocardiogram, exercise stress test, and cardiac enzymes may be ordered.
Pelvic pain can also be confused with lower stomach or abdominal pain. Some possible causes of pelvic pain include:
Urinary tract infection
Ovarian cyst rupture or torsion
Pelvic inflammatory disease
Endometriosis
Fibroids
Kidney stones or infection
Ectopic pregnancy
Likewise, upper stomach or abdominal pain could stem from the lungs and might be a symptom of pneumonia or pulmonary embolism.
The above list of stomach pain causes is not exhaustive. In the end, don't self-diagnose or self-treat—seek out the advice of a healthcare professional.
Treatment
Treatment of stomach pain depends on the underlying diagnosis.
Lifestyle Treatment Options
Several lifestyle modifications may help manage your condition. For example, in the case of celiac disease, a strictly gluten-free diet is essential to treatment, just as restricting lactose (milk products) ingestion is how most people manage lactose intolerance.
Treating GERD may require several lifestyle changes, such as:
Losing weight if you are overweight or recently gained weight
Elevating the head of your bed (for example, placing a foam wedge underneath the top of the mattress)
Avoiding meals two to three hours before going to bed
Lifestyle behaviors are also at the crux of treating constipation.
They include:
Eating foods high in fiber, such as prunes and breakfast cereals
Drinking 6 to 8 glasses of water per day
Engaging in daily physical activity
These are just a few of many examples.
Medications
Some gastrointestinal-related conditions can be managed with over-the-counter or prescription medications.
Acid-Reducing Medications
The occasional heartburn may be treated with over-the-counter antacids like Tums, Maalox, and Mylanta. GERD, peptic ulcer disease, and gastritis require taking a medication called a histamine blocker or a proton pump inhibitor.13
Laxatives
For constipation-related stomach discomfort, laxatives may be recommended by your healthcare provider, particularly if lifestyle changes are not helping. Discuss which laxative to take with your healthcare provider, as they work differently and some may not be safe for you.
Antibiotics
For infectious-related sources of abdominal pain, like diverticulitis, or for the management of H. pylori (when it is the culprit behind a person's gastritis or peptic ulcer disease), antibiotics will be prescribed. While oral antibiotics for H. pylori and mild diverticulitis can be taken at home, moderate-to-severe cases of diverticulitis require hospitalization with antibiotics given through the vein.19
Steroids and Immunosuppressants
Treatment of inflammatory bowel disease may involve steroids and immunosuppressants to slow the progression of the disorder.27
IBS Medications
Treatment of IBS is complex and may entail taking one or more medications, depending on a person's unique symptoms. While not an exhaustive list, some medications used to ease the symptoms of IBS include:
Anti-diarrheal drugs like Imodium (loperamide)
Anti-constipation drugs like Miralax (polyethylene glycol)
Antispasmodics like Bentyl (dicyclomine)
Tricyclic antidepressants like Elavil (amitriptyline)
Surgery
While surgery is the first-line treatment for some gastrointestinal conditions, such as appendicitis, symptomatic gallstones, and abdominal wall hernias, it may be the last resort option for other gastrointestinal problems. For example, a surgery called a Nissen fundoplication may be recommended for refractory GERD.28
Surgery may also be indicated for complications that occur as a result of a gastrointestinal condition—for instance, a perforated peptic ulcer (when a hole forms in the stomach or small intestines) or abscess formation in acute diverticulitis.
Summary
The gastrointestinal system involves numerous organs. Issues with any of these organs can lead to pain in various parts of the abdomen, including the stomach. Stomach pain can also be confused with pelvic pain or heart issues. Furthermore, symptoms of milder conditions like IBS or gallstones can overlap with symptoms of life-threatening conditions like appendicitis or cancer.
For this reason, any time you have sudden or severe pain in the chest, pelvic area, or abdomen, it's important to seek immediate medical attention. Passing dark, tarry stool or vomiting blood warrants an immediate trip to the emergency room as well.
Sources
Johns Hopkins Medicine. Upper gastrointestinal series.
National Institute of Diabetes and Digestive and Kidney Diseases. About the lower GI tract.
Penn Medicine. Peptic ulcer disease.
Fashner J, Gitu AC. Diagnosis and treatment of peptic ulcer disease and H. pylori infection. Am Fam Physician. 2015;91(4):236-42.
Johns Hopkins Medicine. Gastritis.
Stein B, Everhart KK, Lacy BE. Gastroparesis: A review of current diagnosis and treatment options. J Clin Gastroenterol. 2015;49(7):550-8. doi:10.1097/MCG.0000000000000320
National Institute of Diabetes and Digestive and Kidney Diseases. Symptoms & causes of gastroparesis.
National Institute of Diabetes and Digestive and Kidney Diseases. Acid reflux (GER & GERD) in adults.
Johns Hopkins Medicine. Esophagitis.
Harvard Health. Esophagitis.
Johns Hopkins Medicine. Gallstones.
Johns Hopkins Medicine. Pancreatitis.
Feagan BG, Kahrilas PJ, Jalan R, McDonald JWD. Evidence‐Based Gastroenterology and Hepatology. 4th ed. Hoboken, NJ: John Wiley & Sons; 2019. doi:10.1002/9781119211419
Leonard MM, Sapone A, Catassi C, Fasano A. Celiac disease and nonceliac gluten sensitivity: A review. JAMA. 2017;318(7):647-656. doi:10.1001/jama.2017.9730
Johns Hopkins Medicine. Celiac disease.
Deng Y, Misselwitz B, Dai N, Fox M. Lactose intolerance in adults: Biological mechanism and dietary management. Nutrients. 2015;7(9):8020-35. doi:10.3390/nu7095380
Johns Hopkins Medicine. Constipation.
Mount Sinai. Diverticulosis.
Feuerstein JD, Falchuk KR. Diverticulosis and diverticulitis. Mayo Clin Proc. 2016;91(8):1094-104. doi:10.1016/j.mayocp.2016.03.012
Bhangu A, Søreide K, Di Saverio S, Assarsson JH, Drake FT. Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet. 2015:386(10000);1278-1287. doi:10.1016/S0140-6736(15)00275-5
Fujii T, Watanabe M. Definition and epidemiology of inflammatory bowel disease. Nippon Rinsho. 2017;75(3):357-363.
Johns Hopkins Medicine. Ventral (abdominal) hernia.
Cervellin G, Mora R, Ticinesi A, et al. Epidemiology and outcomes of acute abdominal pain in a large urban emergency department: Retrospective analysis of 5,340 cases. Ann Transl Med. 2016;4(19):362. doi:10.21037/atm.2016.09.10
Gans SL, Pols MA, Stoker J, Boermeester MA. Guideline for the diagnostic pathway in patients with acute abdominal pain. Dig Surg. 2015;32(1):23-31. doi:10.1159/000371583
Levine MS, Rubesin SE. History and evolution of the barium swallow for evaluation of the pharynx and esophagus. Dysphagia. 2017;32(1):55-72. doi:10.1007/s00455-016-9774-y
Muthusamy VR, Lightdale JR, Acosta RD, et al. The role of endoscopy in the management of GERD. Gastrointest Endosc. 2015;81(6):1305-10. doi:10.1016/j.gie.2015.02.021
Gionchetti P, Rizzello F, Annese V, et al. Use of corticosteroids and immunosuppressive drugs in inflammatory bowel disease: Clinical practice guidelines of the Italian Group for the Study of Inflammatory Bowel Disease. Dig Liver Dis. 2017;49(6):604-617. doi:10.1016/j.dld.2017.01.161
Oor JE, Roks DJ, Broeders JA, Hazebroek EJ, Gooszen HG. Seventeen-year outcome of a randomized clinical trial comparing laparoscopic and conventional Nissen fundoplication. Ann Surg. 2017;266(1):23-28. doi:10.1097/SLA.0000000000002106
Additional Reading
Macaluso CR, McNamara RM. Evaluation and Management of Acute Abdominal Pain in the Emergency Department. Int J Gen Med. 2012;5:789-97. doi:10.2147/IJGM.S25936.
Penner RM, Fishman MB. (2017). Evaluation of the adult with abdominal pain. Auerbach AD, Aronson MD, eds. UpToDate. Waltham, MA: UpToDate Inc.

By Barbara Bolen, PhD
Barbara Bolen, PhD, is a licensed clinical psychologist and health coach. She has written multiple books focused on living with irritable bowel syndrome.







Post comments