
by First Hospital of Jilin University
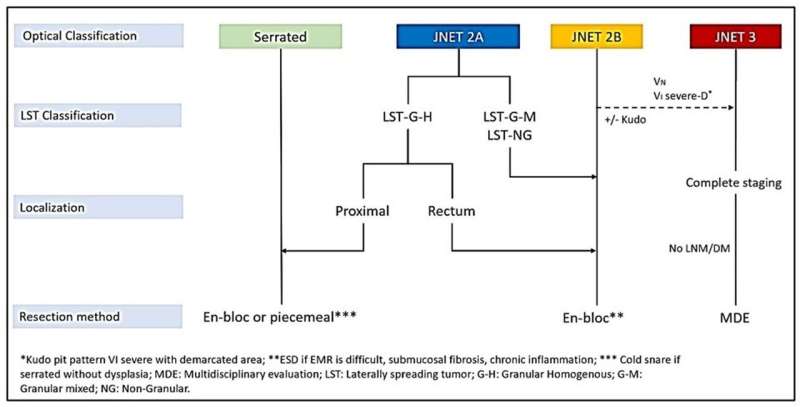
The figure was derived from'International consensus on the management of large (≥20 mm) non-pedunculated colorectal polyps: A World Endoscopy Organisation Delphi study'; Djinbachian et al, 2023; Under review). DM, distant metastasis; EMR, endoscopic mucosal resection; ESD, endoscopic submucosal dissection; JNET, Japan NBI Expert Team; LNM, lymph node metastasis; NBI, Narrow-Band Imaging. Credit: By Taghiakbari M, Kim DHD, Djinbachian R, et al.
Colorectal cancer (CRC) is the second most common cancer in the United States. This highlights the importance of early detection and treatment of precancerous lesions like large polyps. Endoscopy offers a minimally invasive approach to removing these polyps, reducing the need for traditional surgery.
This review, published in eGastroenterology, explores advancements in endoscopic resection techniques, specifically Endoscopic Mucosal Resection (EMR) and Endoscopic Submucosal Dissection (ESD).
Complete removal of large polyps (>10 mm) is crucial to prevent progression to CRC. Piecemeal resection during endoscopic procedures can increase the risk of recurrence. EMR, the standard approach for large, non-pedunculated polyps, utilizes submucosal injection to create a cushion, allowing for safer and more complete resection with a snare.
ESD, a more advanced technique, is employed for complex polyps with a higher risk of submucosal invasion. It involves creating a precise incision and dissecting the polyp layer by layer from the underlying tissue.
Both EMR and ESD offer advantages over surgery. They are less invasive, require shorter recovery times, and are associated with fewer complications. However, selecting the most suitable technique depends on various factors, including polyp size, morphology, location, and depth of submucosal invasion. EMR is generally preferred for simpler polyps, while ESD is indicated for those with features suggestive of deeper invasion.
ESD offers several benefits over EMR. It achieves higher rates of en-bloc resection (removing the entire polyp in one piece), leading to more accurate histological assessment and a lower risk of recurrence. However, ESD is a more complex and time-consuming procedure requiring hospitalization and carries a slightly higher risk of complications. Endoscopic expertise is paramount for successful ESD, with studies showing a significant improvement in success rates with increasing experience.
The choice between EMR and ESD should be individualized based on the patient's specific needs, polyp characteristics, and the available expertise at the treatment center. In some cases, particularly in facilities with limited ESD experience or when delays due to complex procedures could outweigh the benefits, EMR might be the preferred approach.
In conclusion, EMR and ESD are valuable endoscopic techniques for managing large colorectal polyps. Selecting the most appropriate procedure requires careful consideration of individual factors and the endoscopist's skillset. Ongoing research will refine these techniques and guide optimal treatment decisions for patients with precancerous colorectal lesions.
More information: Mahsa Taghiakbari et al, Endoscopic resection of large non-pedunculated colorectal polyps: current standards of treatment, eGastroenterology (2024). DOI: 10.1136/egastro-2023-100025
Provided by First Hospital of Jilin University






Post comments