
by Society for Academic Emergency Medicine
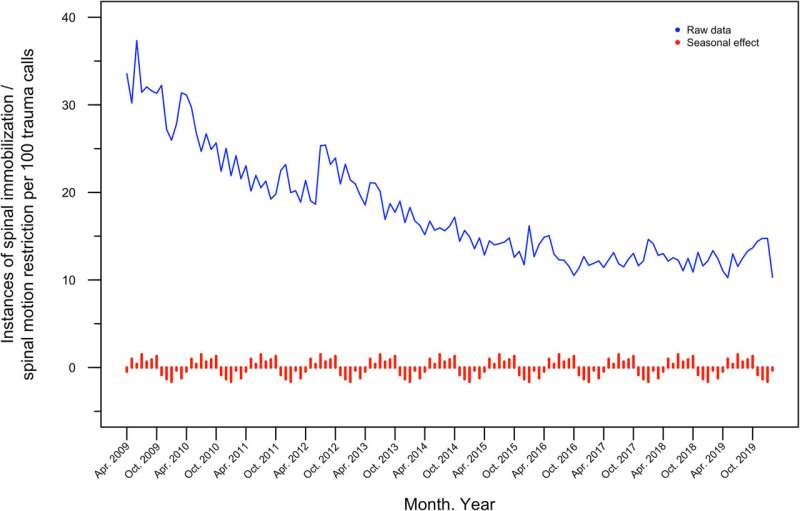
Time series of prehospital SI/SMR. Raw data plotted by month, 2009–2020. Seasonal effect averaged for each month over the study period, showing the monthly maximum (1.4, July) and minimum (−1.6, January). SI, spinal immobilization; SMR, spinal motion restriction. Credit: Academic Emergency Medicine (2023). DOI: 10.1111/acem.14678
A study analyzing the practice of spinal motion restriction (SMR) between 2009 and 2019 has been published in the July issue of Academic Emergency Medicine (AEM). The study, titled Patterns of Change in Prehospital Spinal Motion Restriction: A Retrospective Database Review, sheds light on the trends and evolution of SMR practices within one urban, North American EMS agency.
Key findings from the study include a significant decrease in the prehospital use of cervical immobilization and backboards between 2009 and 2019. Particularly noteworthy was the decline in the combination of cervical immobilization and backboard use, which decreased from 31% to 12% over the study period. This decline was not attributed to protocol changes but rather appeared to be part of a secular trend, particularly evident in cases involving minor mechanisms of trauma.
International training guidelines teach the treatment of potential spine injuries as a core skill in both the emergency department and the prehospital environment. During the past decade, however, these guidelines have been substantially revised. Past practice, termed spinal immobilization (SI), most often positioned patients at risk of spine injury supine on a long, rigid backboard and immobilized them with straps, a rigid cervical collar, and head blocks. More recently, spinal motion restriction (SMR) acknowledges the adverse effects of immobilization, as well as the limitations of its potential benefits and typically allows more leeway in treatment options depending on patient presentation. Despite widespread adoption of the principles of SMR, practices and specific guidelines vary.
The lead author of this article is Neil McDonald, MPhil, University of Manitoba, and Winnipeg Fire Paramedic Service in Winnipeg, Manitoba, Canada. McDonald et al. conclude that the decreasing trend in SI/SMR treatment needs to be investigated elsewhere. Ongoing research at their EMS practice will investigate how these treatment trends may affect patient outcomes.
More information: Neil McDonald et al, Patterns of change in prehospital spinal motion restriction: A retrospective database review, Academic Emergency Medicine (2023). DOI: 10.1111/acem.14678
Journal information: Academic Emergency Medicine
Provided by Society for Academic Emergency Medicine






Post comments