
by Melissa Rohman, Northwestern University
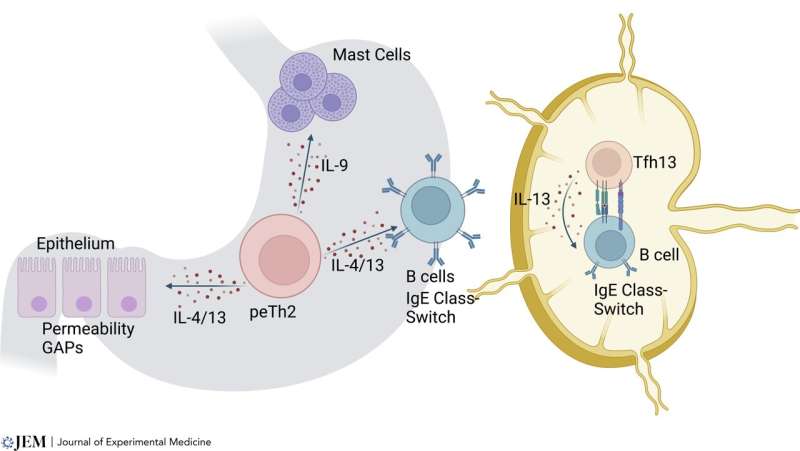
Type 2 cell subsets play diverse roles in the pathogenesis of food allergy. Tfh13 and peTh2 cells have been identified in food allergy. Tfh13 cells are likely responsible for the initiation of class switch and generation of food-specific IgE. peTh2 cells are found in the periphery, and likely play a tissue helper role through promotion of mast cell expansion, increased epithelial permeability to food antigens, and support of local IgE class switch from memory IgG cells. Credit: Journal of Experimental Medicine (2023). DOI: 10.1084/jem.20221104
In her laboratory, Cecilia Berin, Ph.D., the Bunning Professor of Food Allergy Research, studies the immune basis of allergy and tolerance to foods.
In a recent editorial published in the Journal of Experimental Medicine, Berin discusses the current state of treatments for IgE-mediated food allergies (which currently affect roughly 8% of the U.S. population), targeting type 2 immune responses and next steps for food allergy research and treatment development.
What are IgE-mediated food allergies and how are they diagnosed?
The basis of IgE-mediated food allergies lies in a type of antibody called IgE. When these antibodies see the allergens for which they are specific—whether that's pollen, peanuts or something else—the allergens bind to the antibodies and those antibodies activate cells called mast cells or basophils. Those mast cells and basophils release chemicals like histamine that can cause allergic reactions.
Generally, what indicates an IgE-mediated food allergy is timing, that it occurs within minutes up to two hours after exposure. The symptoms are quite standard: hives, respiratory symptoms, nausea and vomiting. Physicians will administer a couple of different tests to check for IgE antibodies. One method is skin testing, where they put a small amount of the food allergen into the skin, and it causes a wheal and flare reaction if there are IgE antibodies present. There are also blood tests that can detect IgE antibodies specific to different foods.
What types of immune responses lead to IgE-mediated allergies?
B-cells can make different kinds of antibodies. They can make IgG antibodies or IgA antibodies that are protective against conditions such as bacterial infection. T-cells —specifically CD4+ T-cells—instruct the B-cell about what kind of antibody to make and CD4+ T-cells make type 2 cytokines that can instruct B-cells to make IgE antibodies. So, before someone has an allergic reaction, they have to already have been exposed to that food or antigen, and during that exposure, there is a generation of a type 2 cytokine response from a type of CD4+ T-cell called the T follicular helper cell that can instruct B-cells to make IgE.
What therapies are available for IgE-mediated food allergies and how effective are they?
There is currently only one FDA-approved treatment and that is for peanut allergy, and it is a treatment called Palforzia, and it's basically a peanut powder that is given in small doses and increases in amount over time as individuals become desensitized to that protein. So, the idea is that ingestion leads to desensitization of mast cells and basophils, it causes a change in the antibodies that are produced against that food allergen, and that leads to protection as long as people continue to take that therapy.
This is pretty effective in desensitizing an individual, so roughly 75% to 80% of individuals will respond to allergen immunotherapy. But the issue is that just like before, they always had to avoid the food. Now they always have to take their medication with taking this immunotherapy in order to maintain the protection that they get. So, it's not a cure.
In your paper, you discuss the need for more precision therapies for IgE-mediated allergies. Please describe these therapies.
One of them is an antibody called dupilumab, which binds to the IL-4 receptor, which is used by two different cytokines, IL-4 and IL-13. These play a very important role in allergic diseases. They are responsible for the B-cell making IgE antibodies, and so the idea is that by blocking those cytokines from binding to their receptors, you can reduce the amount of IgE and also reduce the effect of those cytokines on other aspects of physiology.
This has been tested in two ways. One is as a standalone therapy—giving anti-IL-4 and anti-IL-13—which has not proven to be particularly effective. The other, which is currently being tested, is combining this approach with giving the allergen. The benefit here is that the T-cell and the B-cells are getting activated, but they're getting starved of the cytokine IL-4 and IL-13. So, the idea is that you're going to reprogram the B-cell and the T-cell response because they're no longer getting those Th2 cytokines.
That is also the idea behind the use of JAK inhibitors. JAKs are part of the signaling cascade that is responsible for cytokine receptors having their effects on cells. They target more cytokine receptors than antibodies do. So, the idea is by blocking more cytokines that are involved in allergic disease, they may be more effective at their job.
The precision medicine part of this comes in because we had found in a previous clinical trial of oral immunotherapy that individuals who had a high frequency of Th2 cells—or type two T-cells in peripheral blood—were more likely to fail treatment. They weren't able to get up to the maintenance dose of therapy, and they were less likely to become fully desensitized. If it were possible to test ahead of time whether a patient has a high frequency of these cells, we could perhaps predict whether or not adding dupilumab or a JAK inhibitor to the oral immunotherapy might improve the odds of treatment success.
What are the next steps in food allergy research and treatment development?
I think that there are two key questions. First is identifying who could really benefit from adding on additional therapies. These broader therapies do have more side effects. Inhibiting more cytokines is going to have more side effects than being very targeted. It would be great if we could identify who would respond well to plain oral immunotherapy—then, we could say that they do not need to be exposed to more immunomodulation.
But we may be able to identify those who would respond well versus those who do not. We've also identified these type 2 T-cells. We know that with immunotherapy they get depleted, but when immunotherapy stops, they come back. From an immunology basic science perspective, we need to understand where the memory cells are that can repopulate those pathogenic Th2 cells. Can we prevent those Th2 cells from coming back after we've stopped therapy? That's something that I think still needs more research to understand.
More information: M. Cecilia Berin, Targeting type 2 immunity and the future of food allergy treatment, Journal of Experimental Medicine (2023). DOI: 10.1084/jem.20221104
Journal information: Journal of Experimental Medicine
Provided by Northwestern University






Post comments