
By James Myhre & Dennis Sifris, MD
Medically reviewed by Lindsay Cook, PharmD
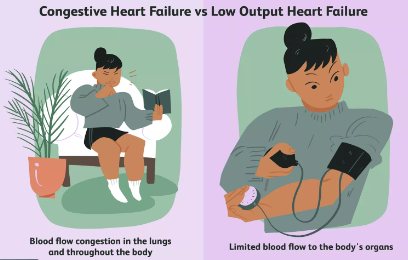
Congestive heart failure (CHF) is the term used to describe what happens when the heart is unable to pump enough blood to meet the body’s needs. (It should not be confused with cardiac arrest in which the heart stops beating entirely.) CHF is simply the inadequate functioning of the heart muscle. The condition can either be acute (it occurs rapidly), or chronic (it occurs over the long term).
Symptoms of CHF may include fatigue, the swelling of the legs, and shortness of breath (especially with exercise).1 CHF can be diagnosed based on a review of your symptoms, blood tests, a cardiac ultrasound, and X-ray. Treatment can vary by the underlying cause and may include diet, exercise, anti-hypertensive medications, blood thinners, and drugs like Entresto (sacubitril/valsartan) and Jardiance (empagliflozin).
Severe cases may require an implantable cardiac device to improve the strength or rhythm of the heart. In the worst-case scenario, a heart transplant may be required.
Low output heart failure occurs in people with heart failure who have little or no lung congestion. In these situations, the main problem tends to be that the heart muscle has become so extremely weak that the heart is no longer able to pump enough blood to the body's organs.
People whose heart failure is primarily low output heart failure are more likely to have low blood pressure, lightheadedness, and syncope (fainting). Low output heart failure is usually a sign of very advanced heart failure and is associated with a very poor prognosis.
Congestive Heart Failure Symptoms
The symptoms of CHF can vary by the location of the heart damage, broadly described as left-sided heart failure, right-sided heart failure, or biventricular failure.
Left-Sided Failure
The left side of the heart is responsible for receiving oxygen-enriched blood from the lungs and pumping it to the rest of the body.
If the heart is failing on the left side (referred to as left ventricular heart failure), it will back up into the lungs, depriving the rest of the body of the oxygen it needs.
Left-sided heart failure is either caused by systolic dysfunction, which is when the heart doesn’t pump out blood the way it should, or diastolic dysfunction, in which the heart doesn’t fill up with blood as it should.2
Characteristic symptoms of left-sided heart failure include:
Fatigue
Dizziness
Shortness of breath, especially when lying flat or during exertion
Dry hacking or wheezing
Rales and crackling sounds in the lungs
Abnormal "galloping" heart sounds (gallop rhythm)
Nighttime breathlessness (paroxysmal nocturnal dyspnea)
Cool skin temperature
Bluish skin tones due to the lack of oxygen (cyanosis)
Confusion
Right-Sided Failure
The right side of the heart is responsible for receiving oxygen-poor blood from the body and pumping it to the lungs to be oxygenated.2
If the right side of the heart is failing (known as right ventricular heart failure), the heart cannot fill with enough blood, causing the blood to back up into the veins.
Right-sided heart failure is often caused by pulmonary heart disease (cor pulmonale) in which the enlargement or failure of the right ventricle leads to circulatory congestion in the lungs as well as the rest of the body.3
Characteristic symptoms of right-sided heart failure include:
Fatigue
Weakness
Shortness of breath, particularly with exercise
Accumulation of fluid, usually in the lower legs (peripheral edema) or lower back (sacral edema)
A distended jugular vein in the neck
Rapid heart rate (tachycardia)
Chest pain or pressure
Dizziness
Chronic coughing
Frequent nighttime urination (nocturia)
The build-up of fluid of the abdomen (ascites)
An enlarged liver
Nausea
Loss of appetite
Biventricular Failure
Biventricular heart failure involves the failure of both the left and right ventricles of the heart. It is the type most commonly seen in clinical practice and will manifest with symptoms characteristic of both left and right heart failure.4
One of the common features of biventricular heart failure is pleural effusion, the collection of fluid between the lung and chest wall.
While pleural effusion can occur with right-sided heart failure and to a lesser extent with left-sided heart failure, it is far more characteristic when both sides are involved. Symptoms of pleural effusion include:
Sharp chest pain
Shortness of breath, particularly with activity
Chronic dry cough
Fever
Difficulty breathing when lying down
Difficulty taking deep breaths
Persistent hiccups
Complications
CHF is a potential complication of many different diseases and disorders. However, the development of CHF can spur further complications, increasing the risk of illness, incapacitation, and death. Characteristic complications of CHF include:
Venous thromboembolism, which is a blood clot that forms when blood starts to pool in a vein.5 If the clot breaks off and travels to the lung, it can cause a pulmonary embolism. If it breaks off and lodges in the brain, it can cause a stroke.
Kidney failure, which can occur when reduced blood circulation allows waste products to accumulate in the body. If severe, dialysis or a kidney transplant may be required.
Liver damage. This commonly occurs with advanced right-sided heart failure when the heart fails to supply the liver with the blood it needs to function, leading to portal hypertension (high blood pressure in the liver), cirrhosis, and liver failure.6
Lung damage, including empyema (accumulation of pus), pneumothorax (collapsed lung), and pulmonary fibrosis (lung scarring) which is a common complication of pleural effusion.
Heart valve damage, which can occur as your heart works harder to pump blood, causing the valves to enlarge abnormally. Prolonged inflammation and heart damage can lead to severe arrhythmia, cardiac arrest, and sudden death.
Causes
Causes of CHF include coronary artery disease, high blood pressure, heart valve disease, infection, excessive alcohol use, or a previous heart attack.7
Congestive heart failure (often referred to simply as heart failure) affects around 6 million Americans and is the leading cause of hospitalization in people over 65 years old. Over 650,000 new cases are diagnosed each year.
The word "congestive" refers to the build-up of fluid in the veins and tissues of the lungs and other parts of the body. It is this congestion which triggers many of the characteristic symptoms of CHF.
CHF is caused by any number of conditions that damage the heart muscle itself, referred to as cardiomyopathy. Common causes include:7
Coronary artery disease (CAD), in which the arteries that supply blood and oxygen to the heart become narrowed or obstructed
Myocardial infarction (MI), also known as a heart attack, in which a coronary artery becomes blocked, which starves and kills heart muscle tissues
Heart overload (including high-output heart failure), in which the heart is overworked by conditions such as hypertension, kidney disease, diabetes, heart valve disease, a congenital heart defect, Paget’s disease, cirrhosis, or multiple myeloma
Infections, which includes viral infections such as German measles (rubella) or coxsackie B virus. Another cause is systemic viral infections, such as HIV, which can cause progressive damage to the heart muscle. Non-viral illnesses like Chagas disease can also cause heart failure
Long-term alcohol or substance abuse, including methamphetamine or cocaine abuse
Cancer chemotherapy drugs like daunorubicin, cyclophosphamide, and trastuzumab
Amyloidosis, a condition in which amyloid proteins build up in the heart muscle, often in association with chronic inflammatory disorders like lupus, rheumatoid arthritis, and inflammatory bowel disease (IBD)
Obstructive sleep apnea, a form of sleep apnea considered an independent risk factor for CHF when accompanied by obesity, hypertension, or diabetes
Toxic exposure to lead or cobalt
Acute Decompensated Heart Failure
Chronic heart failure is the stage in which the heart condition is stable. Chronic heart failure can sometimes progress to acute decompensated heart failure (ADHF) in which the symptoms worsen and increase the risk of respiratory failure.8
ADHF if often triggered by an instigating event such as:9
Heart attack
Pneumonia
Uncontrolled or worsening hypertension
Hyperthyroidism (overactive thyroid gland)
Severe anemia
Arrhythmia (abnormal heart rhythm)
Diagnosis
If congestive heart failure is suspected, your healthcare provider will make the diagnosis based on a review of your symptoms, a physical examination, blood tests, imaging tests, and other diagnostics designed to measure heart function. The failure will then be classified by order of severity to direct the appropriate course of treatment.
Physical Examination
After a review of your symptoms and medical history, your healthcare provider will perform a physical exam to identify the symptoms indicative of CHF.10 This will include, among other things, a review of your:
Blood pressure
Heart rate
Heart sounds (to check for abnormal rhythms)
Lung sounds (to assess for congestion, rales, or effusion)
Lower extremities (to check for signs of edema)
Jugular vein in your neck (to check whether it is bulging or distended)
Laboratory Tests
There are a number of blood tests used to diagnose CHF, some of which can identify the underlying cause of the dysfunction. These may include a complete blood count (to check for anemia), a C-reactive protein (to detect signs of infection), and liver function, kidney function, or thyroid function tests (to establish whether other organ systems are involved and why).
Arguably the most important test is the B-type natriuretic peptide (BNP) test which detects a specific hormone secreted by the heart in response to changes in blood pressure. When the heart is stressed and works harder to pump blood, the concentration of BNP in the blood will begin to rise.11
The BNP test is one of the cornerstone diagnostics of heart failure. However, increases in BNP values do not necessarily correspond to the severity of the condition.
In most labs, a BNP of less than 100 picograms per milliliter (pg/mL) can definitively rule out CHF in 98% of cases.
High BNP levels are far less conclusive, although levels above 900 pg/mL in adults over 50 years old can accurately diagnose CHF in around 90% of cases.12
Imaging Tests
The primary imaging tool for diagnosing CHF is an echocardiogram. An echocardiogram is a form of ultrasound that uses reflected sound waves to create real-time images of the beating heart.10 The echocardiogram is used to determine two diagnostic values:
Stroke volume (SV): the amount of blood exiting the heart with each beat
End-diastolic volume (EDV): the amount of blood entering the heart as it relaxes
The comparison of the SV to the EDV can then be used to calculate the ejection fraction (EF), the value of which describes the pumping efficiency of the heart.
Normally, the ejection fraction should be between 55% and 70%. Heart failure can typically be diagnosed when the EF drops below 40%.13
Another form of imaging, known as angiography, is used to evaluate the vascular structure of the heart. If coronary artery disease is suspected, a narrow catheter would be inserted into a coronary artery to inject contrast dyes for visualization on an X-ray. Angiography is extremely useful in pinpointing blockages that may be damaging the heart muscle.
A chest X-ray on its own can help identify cardiomegaly (enlargement of the heart) and evidence of vascular enlargement in the heart. A chest X-ray and ultrasound can also be used to help diagnose pleural effusion.14
Other Tests
In addition to the BNP and echocardiogram, other tests can be used to either support the diagnosis or characterize the cause of the dysfunction. These include:
Electrocardiogram (ECG), used to measure the electrical activity of the heart
Cardiac stress test, which measures your heart function when placed under stress (usually while running on a treadmill or pedaling a stationary cycle)
CHF Classification
If congestive heart disease is definitively diagnosed, your cardiologist would classify the failure based on a review of your physical exam, lab findings, and imaging test. The aim of the classification is to direct the appropriate course treatment.
There are several classification systems a healthcare provider may rely upon, including the functional classification system issued by the New York Heart Association (NYHA) or the CHF staging system issued by the American College of Cardiology (ACC) and the American Heart Association (AHA).
The NYHA functional classification is broken down into four classes based on both your physical capacity for activity and the appearance of symptoms.15
Class I: no limitation in any activities and no symptoms from ordinary activities
Class II: mild limitation of activity and no symptoms with mild exertion
Class III: marked limitation of activity and symptoms at all times except rest
Class IV: discomfort and symptoms at rest and with activity
The ACC/AHA staging system provides greater insight as to what medical interventions should be implemented at which stages.13
Stage A represents those at risk for heart failure, but with no active disease or symptoms. Stage A treatment focuses on prevention through lifestyle changes and medication.
In Stage B, which is considered "pre-heart failure", there is structural disease but no other symptoms of heart failure. This stage is treated with more aggressive medications or surgery in addition to lifestyle changes.
In Stage C, a person has structural disease and symptoms of heart failure. Treatment in stage C focuses on relieving symptoms and preventing further damage.
Stage D is an advanced disease state characterized by recurrent hospitalizations despite attempts to optimize treatment. Treatment for this stage may require a heart transplant or palliative care.
The ACC/AHA system is especially useful—each stage corresponds to specific medical recommendations and interventions.
Treatment
The treatment of congestive heart failure is focused on reducing symptoms and preventing the progression of the disease. It also requires treatment for the underlying cause of the failure, whether it be an infection, a heart disorder, or a chronic inflammatory disease.
The treatment will be largely directed by the staging of the CHF and may involve lifestyle changes, medications, implanted devices, and heart surgery.7
Lifestyle Changes
One of the first steps in managing CHF is making changes in your life to improve your diet and physical fitness and to correct the bad habits that contribute to your illness. Depending on the stage of the CHF, the interventions may be relatively easy to implement or may require a serious adjustment of your lifestyle.16
Reduce Sodium Intake: This not only includes the salt you add to food, but also the types of food that are high in sodium. The less salt in your diet, the less fluid retention there will be. Most healthcare providers recommend no more than 2,000 milligrams per day from all sources.
Limit Fluid Intake: This can vary depending on the severity of your condition, but generally speaking, you would limit your fluids to no more than 2 liters (8.5 cups) per day.
Achieve and Maintain a Healthy Weight: If you are overweight, you may need to work with a nutritionist to first determine your ideal weight and daily calorie intake, and then to design a safe and sustainable low-sodium diet.
Stop Smoking: There is no safe amount of smoking. Smoking contributes to the development of atherosclerosis (hardening of the arteries), making your heart work much harder than it normally would have to.16
Exercise Regularly: You need to find an exercise plan you can sustain and build upon to get stronger. Try starting with no less than 30 minutes of exercise three times per week, incorporating cardio and strength training. Working with a personal trainer can help ensure the appropriate workout routine, which is one that neither overtaxes you nor leaves you unchallenged.
Reduce Alcohol Intake: While an occasional drink may not do you any harm, moderate alcohol intake can sometimes complicate left-sided heart failure, particularly in people with alcohol-induced cardiomyopathy.17 Speak to your healthcare provider about the appropriate limits based on the nature and severity of your CHF.
Medications
There are a number of medications commonly prescribed to improve the function of your heart. These include:13
Diuretics (water pills) to reduce the amount of fluid in your body and, in turn, your blood pressure
Angiotensin-converting enzyme (ACE) inhibitors, which block an enzyme that regulates blood pressure and salt concentrations in your body
Angiotensin receptor blockers (ARBs), which reduce blood pressure by relaxing blood vessels and improving blood flow
Entresto (sacubitril/valsartan), which is a combination drug used in place of ARBs and ACE inhibitors in people with a reduced EF (generally under 40%)
Sodium glucose co-transporter 2 (SGLT2) inhibitors like Jardiance (empagliflozin), which reduce the risk of cardiovascular death and hospitalization in adults with heart failure
Apresoline (hydralazine) and isosorbide dinitrate, which are sometimes prescribed in combination for people who can't tolerate ARBs and ACE inhibitors
Lanoxin (digoxin), which is sometimes prescribed for people with severe heart failure but is largely avoided due to the high degree of toxicity
Vasopressin receptor antagonists like Vaprisol (conivaptan), which may be used for people with ADHF who develop abnormally low sodium levels (hyponatremia)
Beta-blockers, which continue to be an integral component in treating CHF
Ivabradine (Corlanor), which may be prescribed to certain people with stable, chronic heart failure to help reduce heart rate
Drugs to Avoid: There a number of drugs that you may need to avoid if you have heart failure, which may either undermine therapy or contribute to cardiac congestion. These drugs include:18
Nonsteroidal anti-inflammatory drugs (NSAIDs) like Voltaren (diclofenac), Advil (ibuprofen), or Aleve (naproxen) can precipitate fluid retention. Use Tylenol (acetaminophen) instead.
Certain anti-arrhythmia drugs (particularly sodium channel-blocking drugs) may increase heart rhythm problems in people with CHF.
Calcium channel blockers can also induce arrhythmia, particularly in people with left-sided systolic failure.
Salt substitutes typically contain potassium which promotes arrhythmia.
Antacids often contain high quantities of sodium and are best avoided.
Decongestants like pseudoephedrine can raise blood pressure and should only be used under the direction of your healthcare provider.
Since other drugs (including ketamine, salbutamol, tamsulosin, and thiazolidinediones) can affect heart function, it is important to advise your practitioner about any drugs you are taking, including supplements and herbal remedies.
Implantable Devices
Heart failure is described when the EF is 40% or less. This means that 40% or less of the blood in your left ventricle leaves the heart with each heartbeat.
If your EF falls below 35% or you experience severe arrhythmia as a result of CHF, your healthcare provider may recommend an implantable device to reduce the risk of illness or death. Different approaches are used for different conditions.19
Automatic implantable cardioverter defibrillators (AICDs), similar to pacemakers, are used to correct arrhythmias as they occur.
Cardiac resynchronization therapy (CRT) involves the synchronization of the right and left ventricles so that they work more effectively.
Cardiac contractility modulation (CCM), approved in Europe but not in the United States, is used to strengthen the contraction of the left ventricle with synchronized bursts of electrical stimulation.
The implants are typically inserted beneath the skin of the upper left chest. Before the surgery, medication will be given to make you sleepy and comfortable.
The implantation of a device does not require open-heart surgery, and most people can go home within 24 hours.
Surgery
Surgery may be indicated to repair the underlying or contributing causes of heart failure. This may include repairing or replacing leaky heart valves or performing a coronary artery bypass graft (CABG) to redirect the blood flow around one or more blocked arteries.19
If a heart attack has occurred, surgery is often needed to repair the bulging and thinning of the left ventricular, known as a ventricular aneurysm.
Some surgeries are minimally invasive—accessing the heart through a blood vessel or through the chest without opening the ribcage—while others are open-heart.
If the risk of death is high and a donor's heart is not available, open surgery may be used to implant a ventricular assist device (VAD) into the chest.19 The VAD mechanically pumps blood from the left ventricle to the aorta and is powered by an external battery worn over the shoulder. It is a short-term solution used by healthcare providers when waiting for a donor's heart.
A heart transplant is typically indicated with the EF has dropped below 20% and/or the risk of death within one year is high. Around 3,500 heart transplants are performed around the world each year, more than half of which are performed in the United States.20
People who successfully undergo heart transplant surgery can expect to live an additional 15 years on average.
Coping
Being diagnosed with congestive heart failure doesn't mean that you're going to die or that your heart will suddenly stop. It simply means that your heart is failing to work as well as it is supposed to.
While there is no cure for CHF, there are steps you can take to maintain or improve your heart function.
Weigh Yourself Daily: Changes in your weight may be a sign that your condition is worsening. Start by knowing your "dry weight" (your weight when there no extra fluids in our body) and keep a daily record. Call your healthcare provider if your weight is either 4 pounds more or 4 pounds less than your dry weight in the span of a week.
Take Your Medications Daily: You need to maintain a steady concentration of medications in your bloodstream to sustain the desired effect. Some drugs used to treat CHF have a short drug half-life (including Entresto with a half-life of 10 hours) and must be taken as prescribed without missing any doses. To avoid missed doses, try programming alarm reminders on your cell phone.
Keep Your Healthcare Provider Appointments: People who remain under consistent medical care invariably do better than those who don't. Making and keeping your appointments allows your practitioner to intervene before a medical problem become serious or irreversible.
Check Food Labels: Sodium is hidden in many foods that we eat. Learn how to read product labels and to choose foods low in salt, including lean meats, poultry, fish, fruit, vegetables, eggs, low-fat dairy, rice, pasta, and dry or fresh beans. Avoid canned or packaged foods, and be aware that "reduced-sodium" products may still contain more than you need.
Find Alternative Seasonings: Instead of salt or sodium-rich condiments, season your food with fresh herbs, dried spices, lemon juice, or flavored vinegar.
Plan Ahead When Eating Out: Check the menu online in advance of your reservation, and call ahead to discuss your dietary requirements so that you make the right choices.
Get Help Kicking Bad Habits: Quitting "cold turkey" with cigarettes or alcohol is rarely effective. Speak with your healthcare provider about smoking cessation aids (many of which are fully covered by the Affordable Care Act). If you have a drinking problem, ask your practitioner about support groups or alcohol treatment programs.
Try to Relax: Don't treat your stress with alcohol or sleeping pills. Instead, explore methods of stress relief, including exercise, yoga, or meditation. If you are unable to cope, ask your practitioner for a referral to a therapist who can either help you one-on-one or enlist you in group therapy. Heart failure has also been linked to depression, so addressing your feelings with a mental health professional can be helpful.






Post comments