
by Emily Soelberg,Texas A&M University

Credit: Pixabay/CC0 Public Domain
Blood thinners are often prescribed to prevent life-threatening clots. One type, called direct oral anticoagulants (DOACs), is used to treat a variety of conditions that affect blood vessels, the heart and lungs. But like any medication, they only work if taken and monitored correctly.
When patients receive incorrect dosing, lack proper monitoring or take harmful drug combinations, the result can be serious—and often preventable.
With DOACs, these medication errors can lead toincreased bleeding and blood clots, raising the risk of stroke,heart attackorpulmonary embolism, according to Sara Rogers, PharmD, a clinical assistant professor at the Texas A&M Health Institute of Biosciences and Technology, School of Engineering Medicine and Naresh K. Vashisht College of Medicine and faculty fellow at the Institute for Healthcare Access.
Rogers has been exploring how DOACs are used in underserved communities to uncover ways to protect patients and improve care. Along with her co-investigator, Bader Alghamdi, who is a pharmacy professor from Albaha University in Saudi Arabia, Rogers studied how these warfarin-alternative medications are being prescribed to patients being seen at a clinic in Texas.
As a pharmaceutical substitute, DOACs have grown in preference and are often prescribed over warfarin to certain patients with specific diagnoses. Studies have found thatDOACs are more effectiveand safer than warfarin and may evendecrease the riskof ischemic stroke or systemic embolism and bleeding.
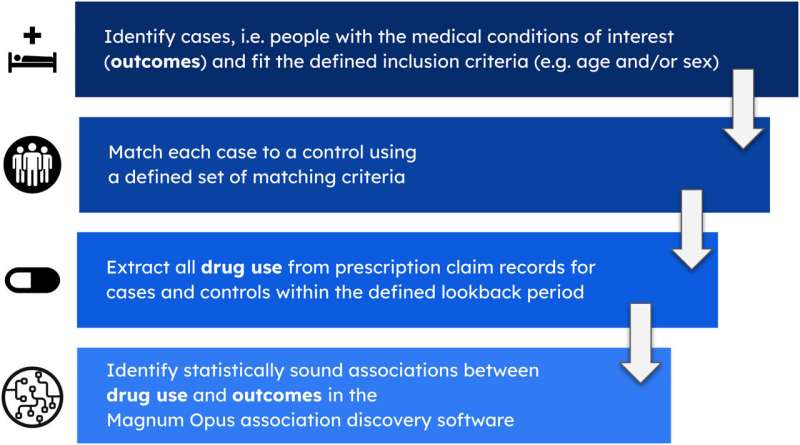
The research team—which included fourth-year pharmacy interns—collected a year's worth of data about patients who were taking an anticoagulant and fit the study's criteria. They assessed the appropriateness of DOAC use and dosing according to guidelines from the Food and Drug Administration (FDA). They also evaluated the inappropriate use of aspirin in combination with DOACs, which has been shown toincrease bleeding—a dangerous risk that may lead to hospitalization.
The study, which was published inScientific Reports, reveals several areas of concern with DOAC prescribing. In 16% of cases, patients received the wrong dose because their kidney function was not properly considered.
Two patients with severe liver disease were prescribed a DOAC, despite the fact that these drugs are not recommended for those conditions. The researchers also found two instances where serious drug interactions led to inappropriate use. Most notably, about two-thirds of the time, patients were taking aspirin alongside a DOAC when the combination was unnecessary.
As a result of these findings, Rogers and Alghamdi argue for a structured anticoagulation stewardship program to support providers working in underserved clinics and help ensure patient safety.
More information: Bader M. Alghamdi et al, Evaluation of gaps in direct oral anticoagulants (DOACs) management in an outpatient underserved clinic: a cross-sectional study, Scientific Reports (2025). DOI: 10.1038/s41598-025-07712-0 Journal information: Scientific Reports
Provided by Texas A&M University





Post comments