
by American Society for Microbiology
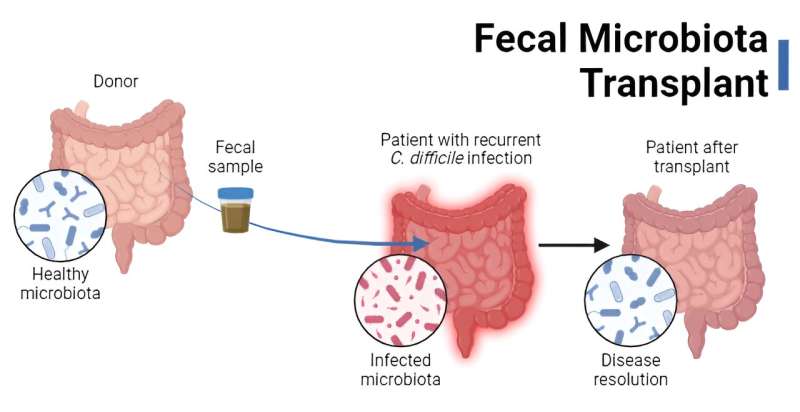
Fecal microbiota transplants are used in the treatment of recurrent C. difficile infection. Credit: American Society for Microbiology
The premise of fecal microbiota transplants (FMT) is, admittedly, not the most pleasant. The process involves transferring donor stool (or derivatives thereof) to a recipient for a therapeutic purpose—namely, to restore the microbiota to a state capable of resisting the gut pathogen Clostridioides difficile.
But where did the idea for FMTs even come from? What's new in the field of transferring feces—and what does the future hold?
It began with feces soup
The birth of FMTs precedes knowledge of microbes, much less the gut microbiota. The first records date back to 4th century China, where "yellow soup" (i.e., human fecal slurry) was used to treat patients with severe diarrhea and food poisoning. Though quite possibly the worst soup ever, it was reported to have "brought patients back from the brink of death."
Fast forward to 1958, when the first "modern" FMT was performed. In this case, fecal enemas were used to cure 4 patients with pseudomembranous colitis, likely caused by C. difficile. Normally, the gut microbiota resists colonization by C. difficile. However, if the microbiota is disrupted, typically following antibiotic treatment for another infection, the pathogen can survive and thrive—secreting toxins, causing diarrhea and damaging the intestine.
The researchers in the 1958 study knew that antibiotics presumably killed off gut microbes and hypothesized that reintroducing "normal" bacteria into the gut via the fecal enemas would "re-establish the balance of nature." The practice wasn't deliberately used for C. difficile infection (CDI) until the 1980s, with some success.
Yet, the treatment never took off. Krishna Rao, M.D., M.S., the co-founder and director of the Fecal Microbiota Transplantation program at the University of Michigan, points to a couple of reasons why. For one, there was the "ick" factor—the idea of administering a slurry of feces to people via enema wasn't very appealing to patients or practitioners.
Second, "CDI was a much different disease back then," he said. "It was viewed as a nuisance, not a massive threat and burden on the health care system." (These days, C. difficile causes nearly half a million infections and 30,000 deaths in the U.S. every year). While antibiotics are the standard treatment for CDI, in some cases they don't work, and the infection will come back (recur), leading to a vicious and potentially deadly cycle of disease.
According to Rao, realization of the full threat of CDI in the 2000s—and increasing rates of recurrent disease—helped bring FMT into the light. But a "landmark" 2013 trial exploring the efficacy of FMT for recurrent CDI gave the practice legs.
The trial showed that infusion of donor stool was incredibly effective at treating patients with recurrent CDI, compared to vancomycin administration alone (94% versus 31% cure rate, respectively). In fact, it was so effective that the study was stopped early, and FMTs were administered to patients in other treatment arms because not doing so was considered unethical.
Later that year, the U.S. Food and Drug Administration (FDA) announced it would exercise enforcement discretion when FMT was used to treat recurrent CDI. That is, patients would not need to receive treatment through a clinical trial, as would be required if FMTs were used for other conditions. This announcement made FMT more accessible to physicians and, ultimately, CDI patients.
How are FMTs used today?
Today, FMT is often reserved for people with recurrent CDI who have failed 2 rounds of antibiotic treatment or have severe disease. The procedure is generally considered safe, and most side effects are transient and localized to the gut (e.g., bloating, constipation, etc.). The cure rate of FMT for recurrent CDI hovers around 80-90% (though analysis of only the most rigorous, controlled clinical trials suggests it might be closer to 70%).
FMTs are (thankfully) not given to patients as a soup these days, and enemas are not the only route of administration. FMTs are also administered via colonoscopy and sometimes with a nasogastric tube (a tube that goes through the nose into the stomach). Donor fecal material can also be encapsulated into pills and taken orally. Regardless of how they are packaged, donor feces are given to patients only after careful screening for various pathogens, including methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus, HIV, and others.
Feces for FMTs are sometimes obtained from stool banks, the largest being OpenBiome, a non-profit organization that collects, screens, and stores stool from healthy donors. Physicians can order fecal material from OpenBiome (or other banks) to administer to patients. For many years, there were no commercial products on the market—until now.
The rise of commercial FMT products
In Nov. 2022, the FDA approved the first commercial FMT product, RBX2660 (Rebyota), for prevention of recurrent CDI in adults. Prepared from donor stool, each dose is administered rectally. Like standard FMT stool suspensions, the precise mixture of microbes in RBX2660 is undefined.
However, the product does ensure a minimum concentration of some bacteria, such as Bacteroides, which are members of the "normal" microbiota that help resist C. difficile colonization. In a phase 3 trial, RBX2660 was significantly better at preventing recurrent CDI compared with placebo (70.6% success versus 57.5%).
Another advancement came in April 2023 with the FDA approval of SER-109 (Vowst)—the first commercial oral FMT product for recurrent CDI. Unlike RBX2660 and other stool preparations, which contain a hodgepodge of microbes, SER-109 contains only donor-derived spores of Firmicutes bacteria, one of the predominant phyla in the microbiota.
Depletion of these bacteria (e.g., because of antibiotic treatment) can create a metabolic environment that promotes CDI recurrence. Replenishing Firmicutes via SER-109 is postulated to restore colonization resistance against the pathogen. Indeed, in patients with 3 or more instances of CDI in 1 year, SER-109 led to a lower recurrence rate after 8 weeks compared to placebo treatment (12.4% versus 39.8%, respectively).
For Rao, the SER-109 product has some extra perks, including the fact that patients can take the pills at home. "Now, if anyone, no matter where they live in the country, sees a patient that needs this treatment, they can write a script, fill out a form, and [the product] gets shipped to their house," he noted. "That's a complete game changer in terms of availability of this modality."
The FDA stamp of approval for both RBX2660 and SER-109 also has important logistical ramifications. "The fact that these are now FDA approved, and at least have the hope of getting covered by insurance—something that was never the case with the OpenBiome product—is a [huge benefit]," Rao said. And these products don't come cheap; a single dose of OpenBiome costs over $1,600, whereas RBX2660 and SER-109 have sticker prices of $9,000 and $17,500, respectively.
Moreover, the FDA revised its guidelines in 2022 to state that it would exercise enforcement discretion only for stool prepared in health care facilities, not stool banks. This makes acquiring stool a challenge that FDA-approved products may help overcome.
Though FMTs are now the standard of care for recurrent CDI, there are still questions about the practice that will continue to shape its development and potential uses.
How do FMTs work—and who are they for?
Despite the name, the mechanisms of FMT are somewhat of a mystery. The general idea is that FMTs repopulate the intestine with microbes capable of resisting C. difficile. But which microbes are needed—and are they needed at all?
The efficacy of SER-109 suggests that only the spore-forming fraction of the microbiota is required, yet sterile fecal filtrate (i.e., lacking microbes) also restored normal stool habits and eliminated symptoms in patients with CDI. "What we thought was necessary and sufficient [for FMTs to work] turns out not to be," Rao said. "That raises the question, "Well, what are the necessary and sufficient components of feces in order to induce a therapeutic response?" And we still don't know that."
Determining which patients should receive a FMT is also unclear. When the COVID-19 pandemic hit, Rao had to suspend University of Michigan's FMT program for over a year. During that time, he treated patients with antibiotics for longer than normal and leaned into holistic care (e.g., encouraging patients to eat fermented foods, which have anti-inflammatory effects). The kicker: the patients got better—his cure rate was north of 90%.
A multi-faceted treatment approach that includes extended courses of antibiotics and diet, among other components, could be all most patients need to recover. "I don't know why FMT works when it does. I think there are patients who do need the FMT, otherwise they won't get better. But that is a much smaller pool of people than I previously would have thought. And I don't know how to identify that person ahead of time," Rao noted.
Addressing unknown threats
The stool used for FMTs is screened for known pathogens, and though it is possible for some to slip through the cracks, this is rare. The larger concern moving forward is how to deal with unknown pathogen threats.
Take mpox (formerly called monkeypox) as an example. Before the onset of the 2022 global outbreak, the virus was circulating in the population—and stool banks and clinicians didn't know about it, raising the risk of transferring mpox to recipients. Depending on the pathogen, such transmission could be dire. "This threat is only going to be happening more often, and we're only going to see more novel pathogens, not fewer," Rao warned.
An additional concern: there are hazy associations between the gut microbiota and numerous conditions, from diabetes to cancer. It is possible that transferring the microbiota from 1 person into another could increase the recipient's risk for developing these diseases years down the line. Rao ensures that every patient for whom he recommends FMT is aware of this "real and very plausible risk."
There is a national registry that aims to track 4,000 patients receiving FMT for 10 years to "identify potential short-term adverse outcomes and to search for long-term safety concerns." So, in a decade, clinicians might know more—but answers will be based on epidemiologic associations. It will still be nearly impossible to look at the microbial profile of stool and say "I can't give this to patient X, or they will develop condition Y."
Toward defined consortia
The "black box" feature of FMTs is why those within the field envision a future where rationally designed biotherapeutic products with defined, lab-grown microbial consortia are the norm. Such products would be beneficial from a safety and regulatory standpoint. However, reaching that ideal requires taking a reductionist research approach, teasing apart how individual microbes (and their products) interact with the host and each other, and how those interactions might be leveraged for therapeutic use.
This approach takes time. Yet, it is especially important if the goal is to harness microbes to treat conditions where ties to the microbiome are not as clear and causal as for CDI, and where FMTs have shown limited success (e.g., inflammatory bowel disease and irritable bowel syndrome, among others).
In Rao's eyes, the more nuanced the associations with the gut microbiota, the more nuanced the solution needs to be. "We can't just throw stool at people [like we did with CDI] and expect it to work," he said. "That's why I'm excited that people are trying to develop these defined consortia because, for other diseases, that's the only way forward."
Provided by American Society for Microbiology






Post comments