
by First Hospital of Jilin University
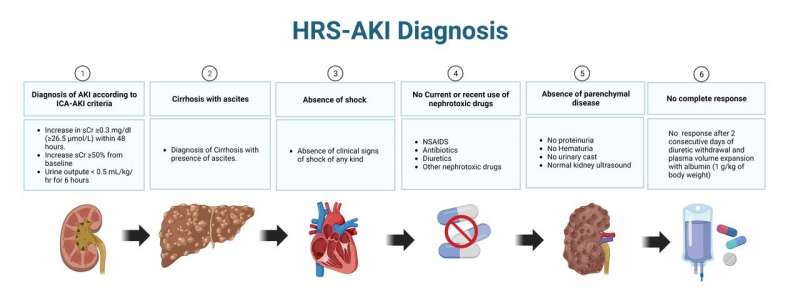
HRS-AKI diagnostic criteria. HRS-AKI is characterized by a decrease in renal blood flow and glomerular filtration rate. It is diagnosed in the context of a patient with cirrhosis with ascites who exhibits reduced renal function but no evidence of intrinsic renal disease, such as haematuria, proteinuria or abnormal renal ultrasound. AKI, acute kidney injury; HRS, hepatorenal syndrome; ICA, International Club of Ascites; NSAIDS, non-steroidal anti-inflammatory drugs; sCr, serum creatinine. Credit: Arnold J, Avila E, Idalsoaga F, et al.
A new study published in the journal eGastroenterology provides an updated assessment of the diagnosis, pathophysiology, and treatment of hepatorenal syndrome-acute kidney injury (HRS-AKI). This severe and often fatal condition can occur in patients with cirrhosis.
HRS-AKI is a functional and progressive kidney failure that is potentially reversible but most often rapidly fatal. It accounts for 11%–20% of all AKI episodes in patients with cirrhosis, and its diagnosis is often challenging to differentiate from prerenal or acute tubular necrosis (ATN).
The study, led by Jorge Arnold, found that early recognition of HRS-AKI is crucial for standard pharmacological treatment with terlipressin plus albumin, restoring kidney function in only 40%–50% of patients.
"In recent years, there has been growing interest in these 'advanced' therapies for managing HRS-AKI," said Jorge Arnold. "On one hand, defining the timing, duration, and modality of renal replacement therapies is crucial. On the other hand, determining the timing and type of transplant needed for each patient's profile presents a major challenge."
The study also found that the timing of when to consider palliative care is an evolving topic.
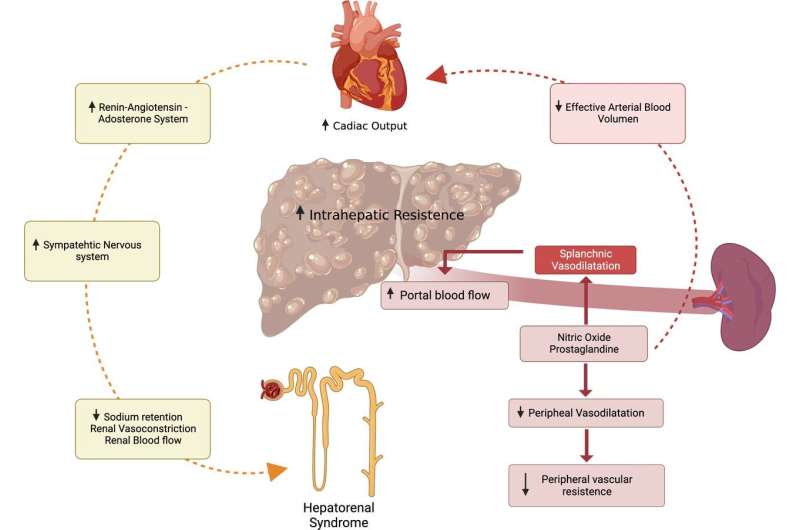
Pathophysiology of hepatorenal syndrome-acute kidney injury. Cirrhosis leads to an elevation in intrahepatic vascular resistance. Splanchnic vasodilation increases the production of vasodilators (nitric oxide, carbon monoxide, prostacyclins and endocannabinoids) within the splanchnic circulation. These vasodilators induce systemic vasodilation, consequently reducing the effective arterial blood volume (EABV) and systemic arterial pressure. To counterbalance this effect, systemic vasoconstrictor pathways, including the renin–angiotensin–aldosterone system, sympathetic nervous system, and arginine vasopressin, are activated to enhance the EABV. However, these compensatory mechanisms lead to sodium retention, impaired solute-free water excretion and renal vasoconstriction, ultimately resulting in reduced renal blood flow. Credit: Arnold J, Avila E, Idalsoaga F, et al.
"Therefore, this review aims to provide an updated assessment of the diagnosis, pathophysiology, and treatment of HRS-AKI, with a particular focus on the benefits and drawbacks of renal replacement therapy (RRT), liver transplantation (LT), combined liver and kidney transplantation (CLKT), and sequential liver-kidney transplantation (SLKT)," said Jorge Arnold.
This study's findings could help improve the care of patients with HRS-AKI and improve outcomes.
More information: Jorge Arnold et al, Advances in the diagnosis and management of hepatorenal syndrome: insights into HRS-AKI and liver transplantation, eGastroenterology (2023). DOI: 10.1136/egastro-2023-100009
Provided by First Hospital of Jilin University






Post comments