
Part of the swallowing process that’s involved in acid reflux and GERD
By Adrienne Dellwo
Medically reviewed by Priyanka Chugh, MD
The lower esophageal sphincter (LES) is a bundle of involuntary muscles—muscles that move or contract without you consciously controlling them. The LES sits right where the lower end of your esophagus—the tube that links your mouth and stomach—connects to the stomach.
The LES is sometimes called the gastroesophageal sphincter or gastroesophageal junction because of the two structures it connects. (“Gastro” means stomach.) It’s sometimes referred to as the cardiac sphincter as well because of its proximity to the heart.
Verywell / Michela Buttignol
The primary job of the LES is to keep the acid and food in your stomach from coming back up into your throat. A weak LES is a common cause of gastroesophageal reflux disease (GERD), in which the esophagus is irritated by stomach acid or bile.
This article discusses the anatomy and function of the lower esophageal sphincter, as well as the diagnosis and treatment of conditions associated with the LES.
How Does the Lower Esophageal Sphincter Work?
The LES is classified as a functional (or physiological) sphincter. Functional sphincters don't have a thickened ring of muscles like anatomical sphincters do. Instead, they have a circular muscle that works by constricting either around or inside of them. This specialized structure can’t be visually identified as a sphincter unless it’s constricted. When it’s relaxed, it looks just like the surrounding tissues.
The LES is also considered an involuntary sphincter. Sphincters are classified as voluntary or involuntary depending on whether you can activate the sphincter consciously or if it’s controlled by involuntary muscles.
Nerve stimulation for involuntary sphincters comes from autonomic nerves, which are part of the autonomic nervous system. It deals with automatic processes, including the function of glands and internal organs.
Structure
The esophagus (also called the gullet) is a tube of muscle that connects your mouth to your stomach. It’s about 8 and 10 inches long and has a sphincter at each end—the upper esophageal sphincter and the lower esophageal sphincter.
A sphincter is a ring of muscle that guards or closes the end of a tube. You have several of them in your digestive system and elsewhere throughout your body. They control the passage of liquids, solids, and gases.
The opening of a sphincter is called the lumen. When the sphincter contracts, the muscle shortens and the lumen closes. When the sphincter muscle relaxes, it lengthens and causes the lumen to open.
Location
The esophagus starts at the bottom of the pharynx (throat). From there, it descends behind the trachea (windpipe) and the heart. It then passes through the diaphragm, which is a membrane that sits just below the lungs.
Just below the diaphragm, at the bottom of the esophagus and top of the stomach, is where you’ll find the LES.
What Are the Other Digestive System Sphincters?
Pyloric sphincter, which is at the lower end of the stomach
Ileocecal sphincter, which is between the small and large intestines
Sphincter of Oddi, which controls secretions from the liver, pancreas, and gall bladder into the duodenum (the first part of the small intestine)
Internal and external anal sphincters, which control the passage of stools from your body
What Does the Lower Esophageal Sphincter Do?
The lower esophageal sphincter remains closed except for when you swallow. Then, it opens to allow food to move down into the stomach.
When you swallow, several structures react to block the airways, so food particles don’t get into your lungs. Food enters the throat, and then both esophageal sphincters open.
After your food goes through the upper esophageal sphincter, the muscles in the esophagus use a wavelike motion (called a peristaltic wave) to then push your food downward and through the LES to the stomach.
The LES stays open for about five seconds after you swallow. It then closes to keep food and digestive enzymes from washing back up into the esophagus.
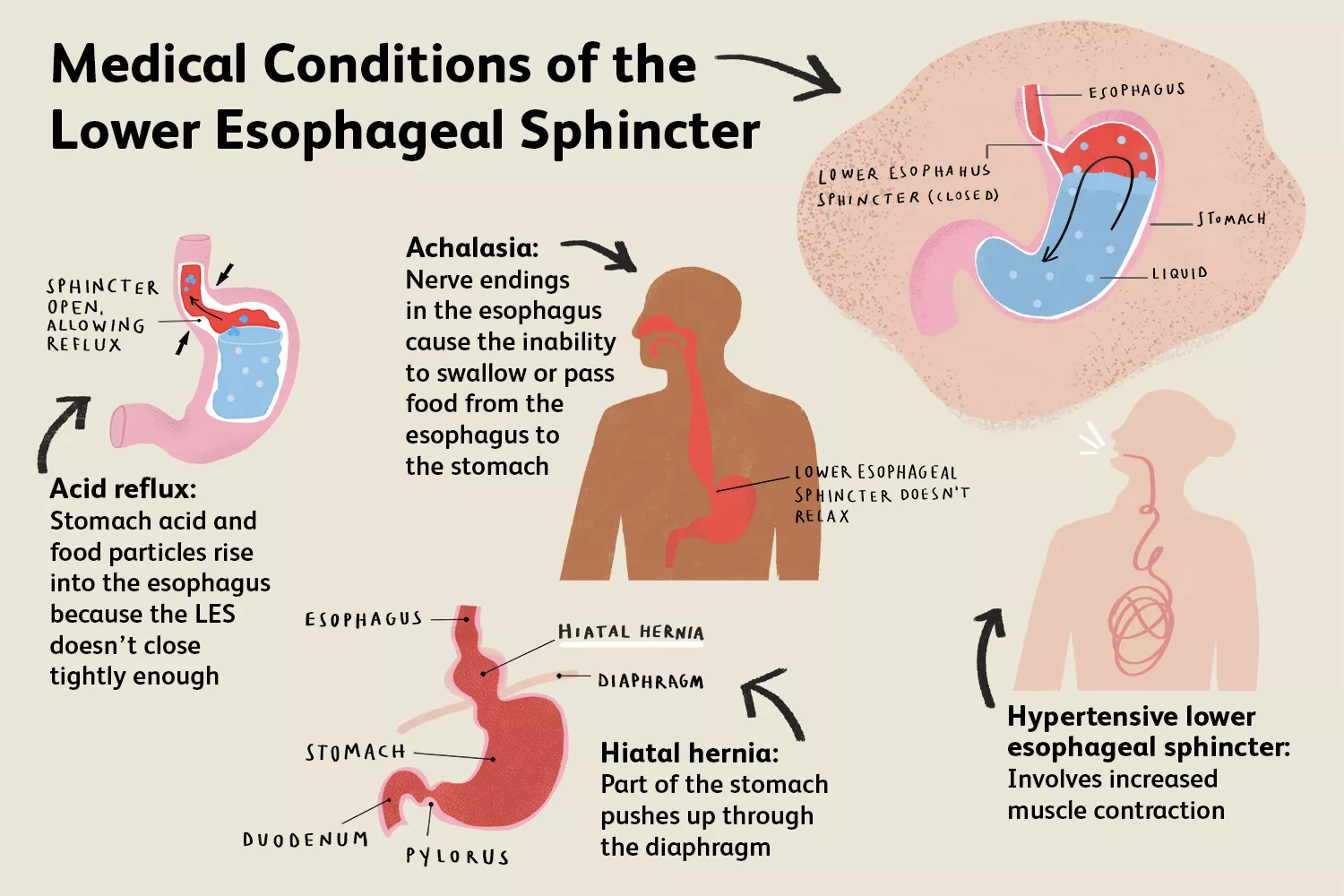
Associated Conditions
Medical conditions involving the LES include:
Acid reflux, heartburn, and gastroesophageal reflux disease (GERD)
Hiatal hernia
Achalasia (an inability to swallow or pass food from the esophagus to the stomach)
Hypertensive lower esophageal sphincter
Acid Reflux, Heartburn, and GERD
When the LES doesn’t close tightly enough, stomach acid and food particles can rise back up into your esophagus. This is called acid reflux.1
The main symptom of acid reflux is heartburn. The burning sensation is actually in your esophagus, but it’s felt in the general vicinity of the heart or in the throat.
Reflux can be brought on by certain foods, alcohol, some medications, pregnancy,2 and an autoimmune disease called scleroderma, which causes hardening and tightening of the skin or connective tissues.3 Acid reflux may get worse when you lie down, especially right after a meal.
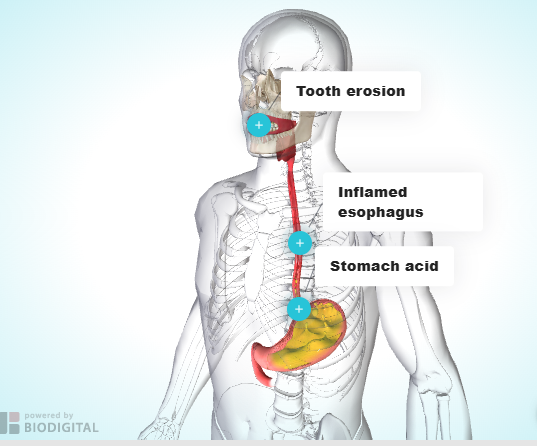
If you have frequent heartburn, it’s important to treat it. Over time, the acid can cause damage to your esophagus.2 GERD is a severe form of acid reflux that can lead to serious complications if it’s not treated.1
Symptoms of GERD typically include:4
Heartburn more than twice a week
Dry cough
Asthma symptoms
Difficulty swallowing
Treatments for acid reflux and GERD can include:
Chewable antacids
Over-the-counter (OTC) acid-reducing medications, such as Pepcid (famotidine)
Prescription acid-reducing medications, such as Prilosec (omeprazole) and Nexium (esomeprazole magnesium)5.
Avoiding problematic foods
Eating small meals
Fasting near bedtime4
Surgery if other treatments aren't effective6
Hiatal Hernia
A hernia is an abnormal protrusion. A hiatal hernia occurs when a part of the esophagus, stomach, or another structure protrudes through the opening where the esophagus passes through the diaphragm.
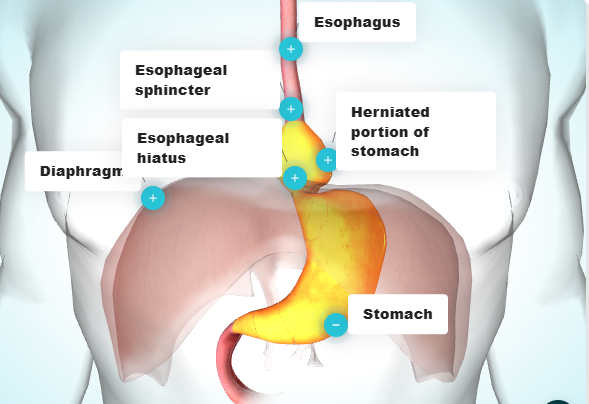
There are four types of hiatal hernia. Type I—the most common—involves the LES moving above the diaphragm instead of being below it, where it belongs. This is also called a sliding hiatal hernia. It can predispose you to GERD.
Type II involves herniation of the stomach. Type III involves the stomach and LES. Type IV involves another organ, such as the colon or spleen.
Causes of hiatal hernia include:7
Chronic coughing
Repetitive vomiting
Pregnancy
Obesity
Straining during bowel movements
Heavy lifting and other types of physical strain
Being born with an unusually large hiatus (opening in the diaphragm)
Injury or trauma to the area such as force from a seatbelt during an accident
Most hiatal hernias cause mild symptoms or no symptoms, so they don’t need to be treated or can be treated with lifestyle changes and over-the-counter antacids or antihistamines. However, if you develop GERD, your hernia does need to be treated.7
In cases where the blood supply is cut off to the herniation, surgery is necessary. It involves pulling the herniated portion out of the diaphragm's hole and closing it.7
The surgeon also strengthens the LES by wrapping the upper part of the stomach around it. This procedure creates a permanently tight sphincter to prevent reflux.7
Achalasia
Achalasia is an inability to swallow or pass food from the esophagus to the stomach. It’s caused by damage to nerve endings in the esophagus, which prevents the peristaltic wave that pushes food down to the LES and keeps the LES from relaxing to allow food through to the stomach.
Symptoms of achalasia include:8
Difficulty swallowing solids and liquids
Regurgitation (food rising up into the throat)
Vomiting
Unintended weight loss
Chest discomfort
This condition can be caused by an autoimmune disease, a viral illness, or, in rare cases, cancer. The cause is usually unknown.9
Treatments for achalasia are aimed at creating an opening in the LES, such as:9
Pneumatic dilation: A catheter and balloon are used to force an opening between muscle fibers through which food can pass into the stomach.10
Heller myotomy: The LES muscle is cut using laparoscopic surgery to make an opening for food to pass through.11
Botulinum toxin (Botox): Botox is injected into the esophagus and LES, which relaxes the sphincter.
So far, no treatments can restore muscle movement in the esophagus.
Muscle relaxants such as Nitrostat (nitroglycerin) or Procardia (nifedipine) may help as well. However, they can be inconvenient, cause unpleasant side effects, and tend to become less effective over time. They’re typically used only when other treatments fail or aren’t an option.9
Hypertensive Lower Esophageal Sphincter
Hypertensive LES involves increased muscle contraction. The cause is often unknown, but it is sometimes related to GERD.12
Symptoms of hypertensive LES often get worse slowly over time. They include:12
Dysphagia (difficulty swallowing)
Chest pain
Heartburn
Regurgitation
Treatment is often myotomy—a minimally invasive surgery similar to that used for achalasia.12
Tests
Diagnostic tests performed for problems related to the lower esophageal sphincter include:
Barium esophagram
Upper endoscopy
Esophageal pH monitoring
Esophageal manometry
Barium Esophagram
An esophagram is a series of X-rays of the esophagus. It can show problems with the LES, poor esophageal emptying, and the lack of a proper peristaltic wave.
Barium is a white, chalky substance that you swallow to make some areas of your body show up better on an X-ray.
Barium esophagrams are often used to diagnose:
Dysphagia
Achalasia
Regurgitation
Hiatal hernia
Leaks
Obstructions
Structural malformations
When the stomach and first portion of the small intestine are included, it’s called an upper gastrointestinal (UGI) series.13
Upper GI Endoscopy
In an upper GI endoscopy, or esophagogastroduodenoscopy (EGD), the esophagus, stomach, and duodenum are examined with a long, flexible tube called an endoscope. It's inserted through the nose or mouth. It’s a common test when a doctor suspects a structural or inflammatory problem.
It’s used to diagnose:
Hiatal hernia
Reflux esophagitis
Masses
Upper GI bleeds
Cancer
While this test can’t diagnose achalasia, it’s usually performed when achalasia is suspected to rule out other possible causes of symptoms.9
Esophageal pH Monitoring
This test is considered the gold standard for diagnosing GERD. It involves 24-hour monitoring of the acid levels in the lower esophagus, near the LES.
It involves placing a thin catheter that detects acid in the esophagus.13 The test reveals how many episodes of high acid you have and how long acid levels are elevated.
Esophageal Manometry
Esophageal manometry involves a small tube with pressure sensors. It’s placed in the stomach via the nose or mouth13 and then slowly withdrawn.
The tube measures pressure at different points along the way. That includes the luminal (opening) pressure in both esophageal sphincters and throughout the esophagus.9
This test is most often used when a doctor suspects:
Achalasia
GERD
Hypertensive LES
Esophageal spasm
How to Treat a Weak Lower Esophageal Sphincter
Treatment of the LES will depend on the condition associated with it and may include:
Chewable antacids
Over-the-counter (OTC) or prescription acid-reducing medications
Muscle relaxant medications
Lifestyle changes, such as avoiding certain foods and adjusting meal timing and sleep position
Botox injection
LES dilation
Surgery
Summary
The lower esophageal sphincter is a ring muscle at the point where the esophagus connects to the stomach. Its job is to stop stomach contents from leaking into the esophagus and mouth. If the lower esophageal sphincter doesn't work properly, you can develop conditions like GERD, in which stomach acid moves back up and irritates the esophagus.
Sources
Johns Hopkins Medicine. Gastroesophageal reflux disease (GERD).
MedlinePlus. Heartburn.
University of California Los Angeles Health. Scleroderma.
MedlinePlus. GERD.
Merck Manual. Medicines for the treatment of gastric acidity.
Johns Hopkins Medicine. Gastroesophageal reflux disease (GERD) treatment.
Johns Hopkins Medicine. Hiatal hernia.
International Foundation for Functional Gastrointestinal Disorders. Disorders of the esophagus.
International Foundation for Functional Gastrointestinal Disorders. Achalasia.
Michigan Medicine. Pneumatic dilation.
University of California San Francisco Department of Surgery. Heller myotomy.
Memorial Hermann Foundation. Hypertensive lower esophageal sphincter.
Johns Hopkins Medicine. FAQs about swallowing disorders.
Additional Reading
National Center for Biotechnology Information, U.S. National Library of Medicine: StatPearls. Physiology, lower esophageal sphincter.
Vogt CD, Panoskaltsis-Mortari A. Tissue engineering of the gastroesophageal junction. J Tissue Eng Regen Med. 2020;14(6):855-868. doi:10.1002/term.3045

By Adrienne Dellwo
Adrienne Dellwo is an experienced journalist who was diagnosed with fibromyalgia and has written extensively on the topic.






Post comments