
by European Alliance of Associations for Rheumatology (EULAR)
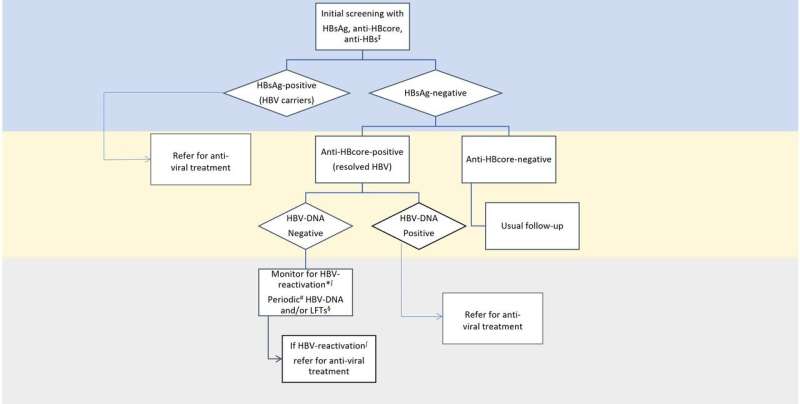
Typical screening for hepatitis B virus (HBV) status include HBsAg, anti-HBcore and anti-HBs. HBsAg-positive patients (HBV carriers) would benefit from prophylactic treatment, and thus it is advised that they should be referred to hepatologist for anti-viral prophylactic treatment. For those who are anti-HBcore-positive and HBsAg-negative (resolved HBV), measurement of HBV-DNA and liver function tests at baseline and then regular monitoring is advised. If HBV reactivation is suspected, based on these tests, referral to hepatologist for anti-viral treatment is recommended. For high-risk patients (eg, commencing treatment with anti-CD20 regimes) prophylactic treatment, irrespective of DNA levels might be considered. ‡Positive anti-HBs without positive HBsAg or anti-HBcore is consistent with prior vaccination. If all three (HBsAg, anti-HBcore, anti-HBs) are negative, means no previous exposure to HBV. *Consider referral for antiviral prophylaxis for those commencing rituximab, having also low titers of anti-HBs. Risk is assessed on an individual basis. ∫HBV-reactivation: rise or appearance of HBV-DNA, or conversion from HBsAg-negative to HBsAg-positive. #Periodic: there are no data to specify the exact time at which re-screening for HBV-reactivation should be performed. However, every 3–6 months is the standard for many national guidelines. Risk factors and cost should also be considered. §Referral to hepatologists is also recommended. Credit: Annals of the Rheumatic Diseases (2022). DOI: 10.1136/ard-2022-223335
It is already known that people who are immunocompromised are more prone to infections. Chronic and opportunistic infections are often found in people with an autoimmune inflammatory rheumatic disease (AIIRD), and may be linked to some of the immunosuppressive and immunomodulatory treatments used to treat these rheumatic diseases. One example of an opportunistic infection that can be more common in people with an AIIRD is tuberculosis (TB).
This infection might not have any symptoms, but can be reactivated, and may spread to other people. There is also a risk of hepatitis reactivation. These infections and reactivations can be prevented with anti-viral treatment or vaccination if they are picked up before starting treatment with disease-modifying antirheumatic drugs (DMARDs), which may suppress the immune system. It is suggested that health care professionals check for these kinds of infections in their AIIRD patients before prescribing DMARDs, but in practice different people's methods vary and there has traditionally been a lack of relevant recommendations.
These new EULAR recommendations were developed by an international task force. This included patient research partners, plus health care professionals with expertise in rheumatology, infections, and respiratory diseases. The information is based on evidence collected from a systematic literature review, which looked at studies on screening and prophylaxis for chronic and opportunistic infections. On the basis of the available evidence, the group drafted a set of potential statements, and voted on their inclusion in the final recommendations.
The paper developed by EULAR and published in November 2022 issue of the Annals of the Rheumatic Diseases includes four overarching principles and eight recommendations. The overarching principles stress that the risk of chronic and opportunistic infections should be considered and discussed with all AIIRD patients before starting treatment with DMARDs, immunosuppressants, or glucocorticoids.
These risks should also be reassessed every so often. People's individual risk factors should be considered in the decision for screening and prophylaxis of chronic and opportunistic infections. To achieve this, there is a need for collaboration between rheumatologists and other medical specialists such as infectious disease doctors, gastroenterologists, hepatologists and pulmonologists. Finally, national guidelines and recommendations should be considered alongside the new EULAR recommendations, as well as possible regional factors that could have a bearing, such as diseases that may be more common in some areas than others.
In this new publication, EULAR now gives guidance and specific recommendations on screening for TB, hepatitis, and HIV in people with an AIIRD before starting DMARD treatment. The recommendations also suggest health care professionals give information and education for people without immunity to varicella zoster so that they understand their risks of getting herpes zoster in the future. There is also a recommendation to give preventative treatment in some patients taking high doses of glucocorticoids to prevent them from getting a pneumocystis pneumonia infection.
The recommendations provide important guidance on how to screen for and prevent chronic and opportunistic infections in people with an AIIRD. EULAR hope their adoption in everyday clinical practice will help to standardize and optimize care, and ultimately reduce the burden of opportunistic infections in people living with AIIRD.
More information: George E Fragoulis et al, 2022 EULAR recommendations for screening and prophylaxis of chronic and opportunistic infections in adults with autoimmune inflammatory rheumatic diseases, Annals of the Rheumatic Diseases (2022). DOI: 10.1136/ard-2022-223335
Journal information: Annals of the Rheumatic Diseases
Provided by European Alliance of Associations for Rheumatology (EULAR)







Post comments