
by Lesley Henton,Texas A&M University
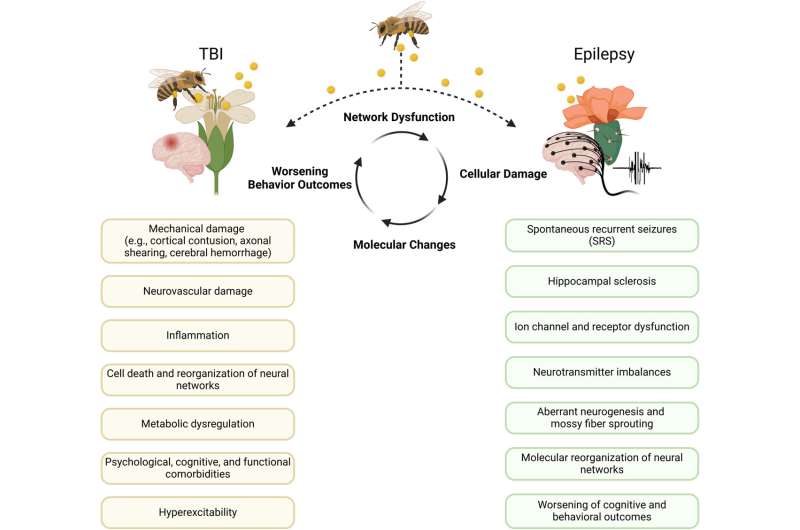
PTE as an interdisciplinary bridge between TBI and epilepsy. Credit:Pharmacological Reviews(2025). DOI: 10.1016/j.pharmr.2025.100080
For decades, researchers have worked to unravel the mysteries of post-traumatic epilepsy (PTE), a form of epilepsy that emerges after a traumatic brain injury (TBI). Now, a new study led by Texas A&M University neuroscientist Dr. Samba Reddy offers a sweeping view of how far the science has come and how far it needs to go.
PublishedinPharmacological Reviews, the study examines howresearch methodshave changed, how scientists find signs of disease, how treatments are developed, and the challenges of turninglab resultsinto real-world therapies. This article is based on the proceedings of the 2023 American Epilepsy Society-supported National Workshop on Experimental Models of Post-Traumatic Epilepsy.
"We've made tremendous strides in understanding the mechanisms that lead to epilepsy after brain injury," said Reddy, Regents Professor of neuroscience and experimental therapeutics and director of the Texas A&M Institute of Pharmacology and Neurotherapeutics. "But the reality is, we still don't have a therapy that can prevent epilepsy from developing. That's the holy grail."
Epilepsy affects more than 80 million people globally, and nearly 40% of those live with seizures that don't respond to medication. PTE accounts for up to 20% of acquired epilepsies and is particularly common among military personnel and civilians who suffer head trauma.
Despite its prevalence, PTE remains difficult to treat. Patients often require multiple medications, and many are not candidates for surgery. The condition can take years to manifest, making early diagnosis and intervention a challenge.
"One of the biggest hurdles is the latent period—the time between injury and the first seizure," Reddy said. "It's a silent window, but it's also our best chance to intervene."
The study reviews dozens of potential therapies, including traditional antiseizure medications, plus cutting-edge approaches like:
"We're moving beyond symptom control," Reddy said. "We're looking at disease modification, changing the trajectory of epilepsy before it starts."
The search for biomarkers—measurable indicators of disease—is another frontier. From examining EEG patterns to molecular markers such as neurofilament light (a protein that helps support nerve cells and can show signs of brain or nerve damage when found in blood or spinal fluid), researchers are identifying ways to predict who will develop epilepsy after TBI.
But the field is still in its infancy.
"We need biomarkers that don't just diagnose epilepsy," Reddy said. "We need ones that can guide treatment and monitor progress."
Reddy explained that sleep disturbances and sex differences play a significant role in PTE. Sleep patterns, especially disruptions in non-REM sleep, may serve as early indicators of the development of epilepsy. Additionally, women often fare better after TBI.
"Women may be less susceptible to PTE due to hormonal protection," he said. "Understanding how sleep and sex hormones interact with brain injury could unlock new therapies."
Despite progress, the road to a cure is long. The study outlines key barriers:
"We need collaboration, funding and standardization," Reddy urged. "Only then can we translate findings into real-world treatments."
The review concludes with eight recommendations to advance PTE research:
"We're at a tipping point," Reddy said. "With the right tools and teamwork, we can move from managingepilepsyto preventing it."
More information: Doodipala Samba Reddy et al, Advances and challenges in experimental models of posttraumatic epilepsy for therapeutic interventions, Pharmacological Reviews (2025). DOI: 10.1016/j.pharmr.2025.100080
Provided by Texas A&M University






Post comments