
by London School of Hygiene & Tropical Medicine
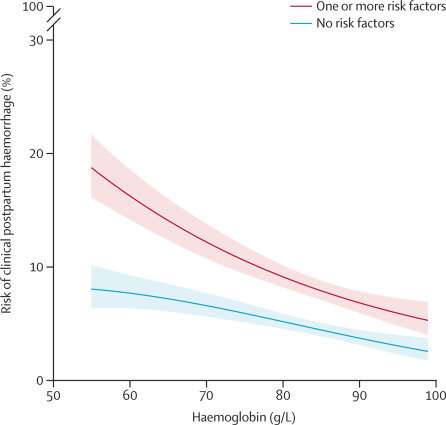
Relationship between hemoglobin and risk of clinical postpartum hemorrhage. The risk of postpartum hemorrhage is calculated using logistic regression with a quadratic term for hemoglobin. The red is the postpartum hemorrhage risk in 4564 women with one or more risk factors (previous postpartum hemorrhage, abnormal placenta, antepartum hemorrhage, infection, multiple pregnancy, and primigravida). The blue line is the risk of postpartum hemorrhage in 5997 women without risk factors. The shaded areas are 95% CIs. Credit: The Lancet Global Health (2023). DOI: 10.1016/S2214-109X(23)00245-0
Pregnant women with anemia are substantially more likely to suffer life-threatening bleeding after childbirth, according to a new study published in the journal The Lancet Global Health.
In a clinical study of more than 10,500 women giving birth in four low-and middle-income countries, a reduction in hemoglobin, the protein in red blood cells that carries oxygen, of 10 grams per liter of blood just before birth increased the risk of life threatening bleeding after childbirth by 23%.
Women with severe anemia (70 grams or less of hemoglobin per liter of their blood) are seven times more likely to die or to become dangerously ill than those with moderate anemia (between 70 and 99 grams of hemoglobin per liter of blood).
Despite the strong association, anemia was not recorded as the cause of severe bleeding in any of the women studied, with the authors stressing that efforts to prevent and treat anemia in women of child-bearing age must be strengthened.
Iron deficiency is the most common cause of anemia. Poor access to a healthy diet, infectious diseases (such as malaria or HIV) and untreated heavy menstrual bleeding are the main causes of iron deficiency in young women.
Severe bleeding after birth, known medically as postpartum hemorrhage (PPH), is the leading cause of maternal death, killing more than 70,000 mothers each year, mostly in low-or middle-income countries.
Links between maternal anemia and PPH have been suggested before but previous studies have been limited by small sample sizes and did not consider different severities of anemia.
In this study, a research team, including from the London School of Hygiene & Tropical Medicine (LSHTM) analyzed data from the ongoing WOMAN-2 clinical trial. In all, 10,561 pregnant women (average age of 27 years old) who were due to give birth vaginally in hospitals in Pakistan, Nigeria, Tanzania and Zambia between 2019 and 2022 were recruited.
Hemoglobin measurements were taken after the women arrived at hospital and just before they gave birth. Doctors assessed whether the new mothers experienced PPH within 24 hours following birth, according to one of three definitions: estimated blood loss of 500 milliliters or more or bleeding sufficient to cause low blood pressure or a rapid pulse (Clinical PPH); estimated loss of 500 milliliters or more (PPH defined by the World Health Organization); calculated estimated blood loss of over 1000 milliliters based on changes in hemoglobin levels and body weight (calculated PPH).
Overall, 742 (7%) of women in the study developed clinical PPH. Those with moderate anemia had a 6.2% chance of experiencing PPH after childbirth, with the risk increasing to 11.2% if their anemia was more severe. According to the study, a 10 gram per liter decrease in the amount of hemoglobin in the blood resulted in a 16% to 23% increase in the likelihood of developing PPH, depending on the definition used. Women with severe anemia were seven times more likely to die or nearly die as a result of severe bleeding than those with moderate anemia.
The authors highlight several limitations of the study, such as potential inaccuracies in estimates of blood loss which they believe may have lessened the observed association between anemia and PPH. As every woman in the trial had either moderate or severe anemia before giving birth, no conclusions can be made about risks for women with milder forms of the condition.
Although such questions will need to be addressed, the authors conclude that the current findings signal the pressing need to not only treat anemia in women of childbearing age but also prevent it if fewer mothers are to lose their lives.
Dr. Ian Roberts, Professor of Public Health at LSHTM, said, "Severe bleeding after childbirth kills one woman every six minutes and anemia greatly multiplies the risk of bleeding and death. Worldwide, half a billion young women are anemic and 20 million are severely anemic. Anemia prevention has been overlooked by the World Health Organization in its efforts to cut deaths from PPH. We need urgent changes in policy and practice."
Obstetrician Professor Rizwana Chaudhri, Head of Translational Research at Shifa Tameer-e-Millat University and lead investigator in Pakistan, said, "We have robust data to show that anemia is an important risk factor for PPH that urgently needs to be addressed before women give birth. The ongoing WOMAN-2 Trial will build on this evidence and find out whether tranexamic acid can be used as an effective intervention for PPH prevention in anemic women."
Raoul Mansukhani, Research Fellow in Medical Statistics at LSHTM, said, "Our study is the first to examine the link between prebirth hemoglobin and PPH in a large sample of women from countries where anemia is common. Our results show that the lower the hemoglobin the higher the risk of severe bleeding and death. Anemia is common and dangerous. Preventing and treating anemia, must be a priority to reduce maternal deaths in these countries and globally."
More information: Raoul Mansukhani et al, Maternal anaemia and the risk of postpartum haemorrhage: a cohort analysis of data from the WOMAN-2 trial, The Lancet Global Health (2023). DOI: 10.1016/S2214-109X(23)00245-0
Read more about the WOMAN-2 trial here.
Journal information: The Lancet Global Health
Provided by London School of Hygiene & Tropical Medicine






Post comments