
by American Association for Cancer Research
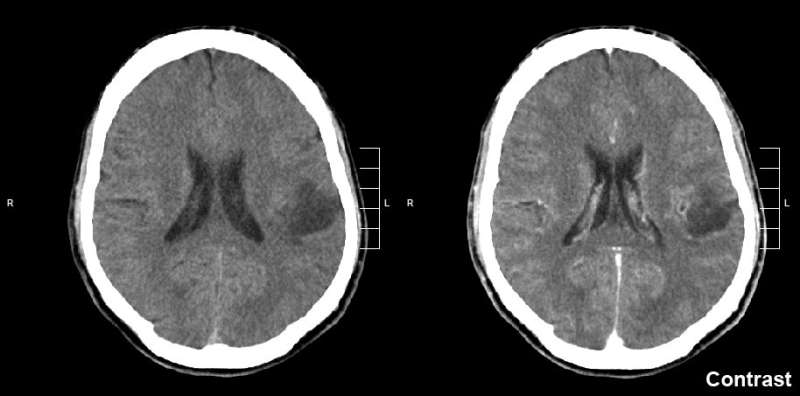
Glioma of the left parietal lobe. CT scan with contrast enhancement. Credit: Mikhail Kalinin/CC BY-SA 3.0
Dabrafenib (Tafinlar), a BRAF inhibitor approved to treat certain types of adult melanoma, showed activity in pediatric patients with low-grade glioma, according to results published in Clinical Cancer Research, a journal of the American Association for Cancer Research.
"Low-grade glioma is the most common brain tumor seen in children. While the prognosis is quite favorable, neurological disability is a major problem," said Darren Hargrave, MD, clinical professor of pediatric neuro-oncology at the Great Ormond Street Hospital in London.
"A major consideration for treatment, particularly in children, is that the brain is a very vulnerable organ," explained Hargrave. "The goal of treatment is to stop the tumor from growing, but we also want to cause the least amount of damage possible to the normal brain."
Patients are often treated with surgery to remove all or part of the tumor, which may be followed by chemotherapy or radiotherapy. While chemotherapy and radiotherapy are both effective treatments, there are trade-offs to each of these options, explained Hargrave. Chemotherapy generally does not cause significant side effects to the normal brain, but patients can experience other severe side effects and admissions to the hospital during the treatment course, which can range from 12 to 18 months. On the other hand, radiotherapy is usually administered for only six weeks, but there is a greater risk of damage to the normal brain. Due to the greater risks of radiotherapy, most patients are initially treated with chemotherapy.
In this phase I/IIa study, Hargrave and colleagues examined the efficacy of an oral targeted therapy called dabrafenib in patients with pediatric low-grade glioma. Dabrafenib selectively inhibits a mutated form of the BRAF protein that causes cell growth. This BRAF mutation is often found in pediatric low-grade gliomas.
"The theoretical advantage of a targeted therapy is that the tumor can be controlled, even shrunk, while causing less damage to normal tissue," said Hargrave. "Limiting the adverse effects on normal tissue has the potential to improve long-term outcomes and treatment burden."
The study enrolled a total of 32 patients, aged one to 18 years, whose tumors had the BRAF mutation. All patients had received at least one prior therapy. Fifteen of these patients were enrolled in the phase I portion of the study, which was also published in Clinical Cancer Research earlier this year, and 17 were enrolled in the phase II portion. All 17 patients in the phase II portion were treated with the recommended phase II dose determined in the phase I study. An additional seven patients in the phase I portion had been treated at this dose. All patients were treated with a pediatric formulation of dabrafenib.
Five patients were not evaluable for objective response but were evaluable and met the criteria for stable disease. Based on independent radiological review, responses were observed in 14 of the 27 evaluable patients. One patient had a complete response, and 13 had partial responses. The median duration of response was 26 months, with a median progression-free survival of 35 months. Eleven patients experienced disease progression.
Treatment-related adverse events were observed in 29 patients, and nine patients experienced grade three or four treatment-related adverse events. There were no treatment-related deaths; however, one patient died two weeks after discontinuing the therapy due to disease progression.
"The number, rapidity, and degree of responses we saw with dabrafenib were higher than what we might expect when treating progressive relapsed pediatric low-grade glioma with chemotherapy," said Hargrave, but he cautioned that results from a randomized phase III study comparing first-line dabrafenib in combination with the MEK inhibitor trametinib and chemotherapy are needed before any direct comparisons can be made. The phase III study is currently open for enrollment.
"If the phase III study shows clinical benefit, dabrafenib could become a new front-line treatment option for pediatric low-grade glioma," Hargrave added. Hargrave and colleagues are also testing trametinib, alone and in combination with dabrafenib, for the treatment of pediatric patients with previously treated low-grade glioma.
A limitation of the study is the lack of data on long-term side effects. Additionally, the study design did not allow researchers to determine the optimal duration of treatment. Another study currently in development will aim to collect these data.
More information: Mark W. Kieran et al. A Phase I and Pharmacokinetic Study of Oral Dabrafenib in Children and Adolescent Patients with Recurrent or Refractory BRAF V600 Mutation–Positive Solid Tumors, Clinical Cancer Research. DOI: 10.1158/1078-0432.CCR-17-3572
Journal information: Clinical Cancer Research
Provided by American Association for Cancer Research






Post comments