
by Matthew Tontonoz, Memorial Sloan Kettering Cancer Center
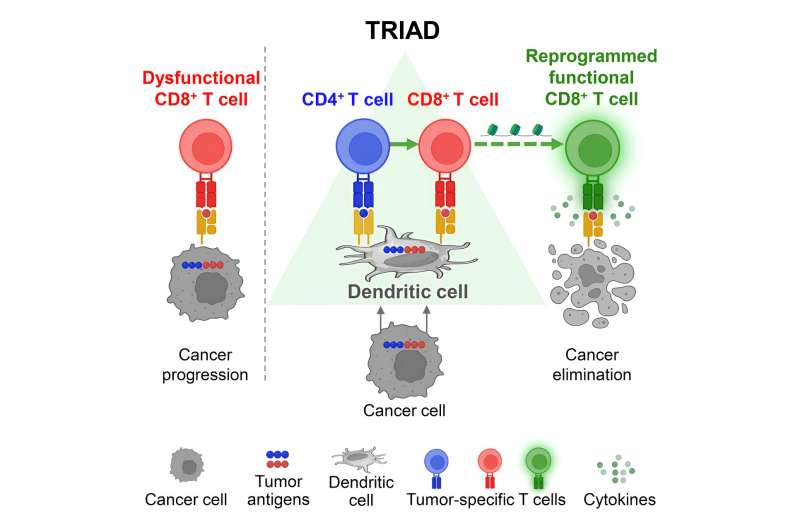
Graphical abstract. Credit: Cancer Cell (2024). DOI: 10.1016/j.ccell.2024.05.025
There's a frustrating fact about today's immunotherapies for cancer. While sometimes they work beautifully—completely eliminating or greatly reducing cancer in particular patients—other times they don't work at all. It's a mystery.
Scientists have posed several hypotheses to explain the disparity. Perhaps it's the number of mutations present in a tumor, with more mutations leading to better responses. Or maybe it's the tissue environment surrounding the tumor, with some environments supporting and others suppressing effective immune responses. But so far, none of these explanations has proved definitive or applicable in all cases.
Researchers at Memorial Sloan Kettering Cancer Center (MSK) and Baylor College of Medicine in Houston, Texas, now think they have a better explanation.
"It turns out that in order for immune cells to effectively kill the cells of a tumor, they need to take on a specific spatial configuration," says Andrea Schietinger, Ph.D., a tumor immunologist and member of the Immunology Program in MSK's Sloan Kettering Institute. "They need to form a triad."
Triad—meaning three cells. But not just any three cells will do. What you need, she explains, is three different immune cells all collaborating together at the same time and in the same spot: one dendritic cell, one cytotoxic ("killer") T cell, and one helper T cell.
These cells aren't rare or unusual, immunologically speaking. They're the standard actors described in any immunology textbook. But up until now, no one knew that these cells needed to be physically present together in tumors in order to generate an effective immune response against cancer cells.
The discovery, which is published in the journal Cancer Cell, has immediate therapeutic implications and could alter the way doctors administer immunotherapies.
Seeking clues about why an elite fighting force fails
A postdoctoral fellow in the Schietinger lab, Gabriel Espinosa-Carrasco, Ph.D., is the first author on the new paper. What sparked Dr. Schietinger's and Dr. Espinosa-Carrasco's curiosity about this line of research was the abundant—and frankly discouraging—data from human clinical trials of adoptive T cell therapies.
These are therapies in which researchers take a sample of cytotoxic T cells from a patient, identify ones that recognize the cancer, then expand those to billions of copies in the lab and return them to the patient. (Alternatively, scientists can engineer T cells in the lab to recognize specific targets and then expand and infuse those.)
The approach sounds logical; it should work, but it often doesn't.
"How is this possible that we can generate the most perfect cytotoxic T cells in the lab, give patients billions of these cells, and yet they still fail to eliminate the cancer?" Dr. Schietinger asks. "There seems to be something so fundamental that we are missing about what cytotoxic T cells need to kill effectively."
In retrospect, she says, the answer seems obvious.
Giving T cells a license to kill
Scientists have known for a long time that cytotoxic T cells don't operate on their own. They need the assistance of helper T cells to become armed and activated. "This is textbook knowledge," Dr. Schietinger points out.
That's why, as she explains, every existing protocol where cytotoxic T cells are being activated and prepared for adoptive T cell therapy adds important chemicals made by helper T cells. At that point, the thinking goes, the cytotoxic T cells should be ready to fight cancer when they are infused back into the body.
But what if cytotoxic T cells need the assistance of helper T cells not only early on to become armed and activated, but also to carry out their kill mission? "Do cytotoxic T cells—like James Bond—need a license to kill?" Dr. Schietinger wondered.
To find out, she and her team devised a mouse model of cancer that she could treat with a form of adoptive T cell therapy similar to those currently used with people. She set up two contrasting situations. In one case, she gave the mice with cancer only cytotoxic T cells. In the other case, she gave the mice both cytotoxic T cells and helper T cells. The results were clear and dramatic: only the mice that had received both types of T cells saw their tumors regress.
"What this implies is that just having the cytotoxic machinery up and running is not really enough to do the actual killing," Dr. Schietinger says. "You need to actually license them to kill the target cell."
How that licensing may occur became clearer when they looked at the tumor tissues from the mice under the microscope. That's when they saw that in the mice that had responded to the treatment, their cells had formed the distinctive immune cell triads. The cells were physically nestled together. Somehow, Dr. Schietinger says, that spatial arrangement allows cytotoxic T cells to finally get the message: time to take action.
It was an interesting and exciting finding. But would it hold beyond the particular mouse model they used?
From mice to humans
To answer that question, Dr. Schietinger and her team reached out to colleagues at Baylor College of Medicine, surgeons Hyun-Sung Lee, MD, Ph.D., and Bryan M. Burt, MD. That group had unpublished data on a group of patients with pleural mesothelioma, a type of lung cancer, who had been treated with a form of immunotherapy called immune checkpoint blockade. Within that group, some of the patients had responded well to the treatment, seeing their tumors shrink, while others did not.
When the surgeons at Baylor went back to look at tissue samples they had collected as part of the trial, they found that those patients who had responded to the therapy had the distinctive triads in their tumors. The ones who didn't respond did not have them.
That was pretty compelling evidence that the immune triads were indeed important, and not just a coincidence. The three types of immune cells interact in such a way that makes them a stronger fighting force against cancer cells.
Clinical implications of immune cell triads
What are the implications of all this? First, says Dr. Schietinger, there is the possibility that these triads could be used as a biomarker for identifying which individuals are likely to respond to immunotherapy. So far, doctors do not have good biomarkers to make that distinction.
Second, the results imply that doctors should rethink how they administer adoptive T cell therapies. Instead of giving predominantly killer T cells, perhaps they should include helper T cells too; and maybe much fewer killer T cells would be enough if there were helper T cells in the mix as well.
Lastly, the results have implications for the design of cancer vaccines, where fragments of cancer-associated proteins are designed to boost patients' killer T cells.
Dr. Schietinger's team is working to advance research in all these directions. For example, one member of her team, a bioengineer, is designing tools to connect one killer T cell to one helper T cell, to encourage their formation of a triad with a dendritic cell (the cell type responsible for presenting fragments of cancer proteins to T cells).
They're also experimenting with new formulations of cancer vaccines and are partnering with other leaders in the field to bring this work to clinical trials.
"The main implication of our findings is that it's not the absolute numbers of cells that matters, it's their spatial configuration," Dr. Schietinger says. "The three cell types need to be on the battlefield together, and building therapeutics which do that is our next big goal."
More information: Gabriel Espinosa-Carrasco et al, Intratumoral immune triads are required for immunotherapy-mediated elimination of solid tumors, Cancer Cell (2024). DOI: 10.1016/j.ccell.2024.05.025
Journal information: Cancer Cell
Provided by Memorial Sloan Kettering Cancer Center





Post comments