
From: Branched-chain amino acid transaminase 1 confers EGFR-TKI resistance through epigenetic glycolytic activation
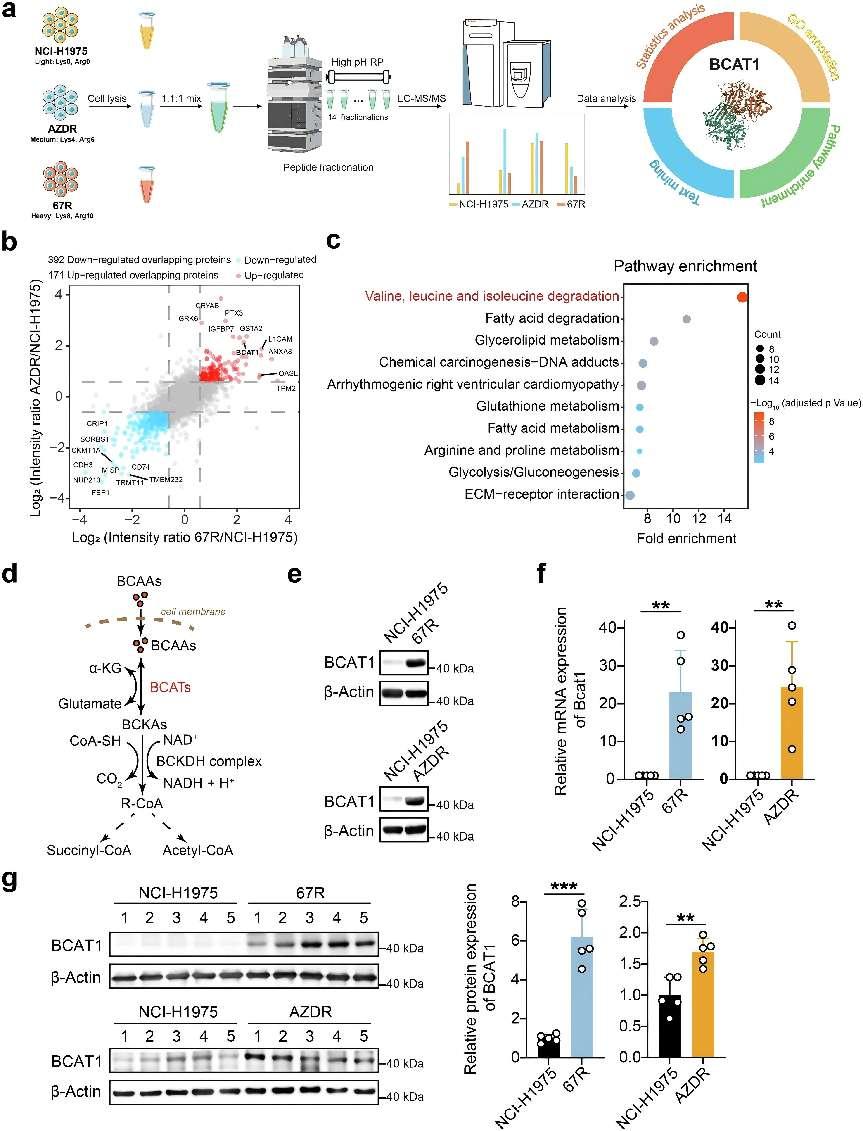
Discovery and validation of enhanced expression of BCAT1 in TKI-resistant lung cancer. a Workflow of the SILAC assay to identify differentially expressed proteins between third-generation EGFR TKI-resistant clones and parental cells. Ribbon representation of the experimental structure of BCAT1 (PDB ID 7NTR42) is shown on the right. b Common differentially expressed proteins in both ASK120067-resistant strains (67R) and osimertinib-resistant strains (AZDR). Red dots: up-regulated overlapping proteins; blue dots: down-regulated overlapping proteins. c Pathway enrichment analysis of differentially expressed overlapping proteins in TKI-resistant cells compared to the parental cells. The top 10 enriched pathways in TKI-resistant cells versus parental NCI-H1975 cells are shown. d Diagram of BCAT-catalyzed reversible BCAAs metabolism. e, f BCAT1 protein levels and relative mRNA levels (n = 5) in the indicated tumor cells were determined by Western blot assay (e) and RT‒qPCR (f). g BCAT1 expression levels in the indicated tumor tissues were determined by Western blot assay (n = 5) and are shown as representative images (left) and a quantitative graph (right). *p < 0.05, **p < 0.01, ***p < 0.001. Data are expressed as the mean ± SD
The development of resistance to epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs) is a leading cause of therapeutic failure and cancer relapse in patients with EGFR-mutated non-small cell lung cancer (NSCLC). The T790M mutation in EGFR exon 20 is the most common cause of resistance to first- and second-generation EGFR TKIs. Third-generation EGFR TKIs, such as osimertinib (AZD9291), are designed to target EGFR with the T790M mutation and other activating mutations, and are widely used in second-line therapy for NSCLC with the T790M mutation and as first-line treatment for NSCLC with EGFR activating mutations. Another third-generation EGFR TKI, ASK120067, has shown promising antitumor effects and is currently under New Drug Application (NDA) review in China. Despite the clinical effectiveness of third-generation EGFR TKIs, resistance eventually emerges through various mechanisms, including EGFR mutations that disrupt drug binding (e.g., C797S), the activation of alternative pathways, abnormal downstream signaling, and lineage plasticity leading to small cell transformation. Over 30% of the resistance mechanisms to osimertinib remain unexplained, prompting the search for new resistance mechanisms and therapeutic strategies for TKI-resistant NSCLC.
Metabolic reprogramming is a key feature of cancer and significantly impacts genome stability, cell proliferation, and the tumor microenvironment. Amino acids are essential for protein synthesis and energy production. Among them, branched-chain amino acids (BCAAs) such as valine, leucine, and isoleucine, are also critical for oncogenesis. Branched-chain amino acid transaminases (BCATs), including cytosolic BCAT1 and mitochondrial BCAT2, initiate BCAA metabolism, which is altered in various cancers, including NSCLC. Upregulated BCAT1 and reprogrammed BCAA metabolism in NSCLC cells have been linked to reduced reactive oxygen species (ROS) accumulation and short-term tolerance to first-generation EGFR TKIs. The precise role of BCAA metabolism in NSCLC progression is not fully understood, and no agents targeting this pathway have been reported for NSCLC treatment.
To uncover these mechanisms, the researchers employed high-throughput proteomics analysis on established TKI-resistant tumor models. They compared the proteomes of osimertinib-resistant (AZDR) and ASK120067-resistant (67R) tumor cells with their parental, TKI-sensitive counterparts (NCI-H1975). This approach revealed a notable upregulation of BCAT1 in both resistant cell lines compared to the parental cells. BCAT1, a cytosolic enzyme involved in branched-chain amino acid (BCAA) metabolism, emerged as a potential mediator of resistance to third-generation EGFR TKIs.
Further investigation confirmed the elevated expression of BCAT1 in both resistant cell lines and xenograft tumors. This upregulation was also observed in TKI-tolerant cells, suggesting its involvement in both acquired and intrinsic resistance. Mechanistically, BCAT1 knockdown or pharmacological inhibition impaired the growth of resistant cells and partially restored their sensitivity to EGFR TKIs.
Subsequently, the researchers explored the role of BCAT1 in BCAA metabolism using stable isotope tracing. They found that BCAT1 knockdown in 67R cells decreased the ratio of labeled BCAA metabolites, indicating a shift towards BCAA anabolism. This led to a decrease of alpha-ketoglutarate (α-KG) content in resistant cells, which is a crucial metabolite involved in various cellular processes, including metabolic reprogramming, signaling, and genetic regulation. This is because BCAT1 can transfer the amino group from BCAAs to α-KG, generating glutamate and the corresponding branched-chain keto acids (BCKAs).
The mechanisms by which α-KG contributes to drug resistance are not well-defined. One possible mechanism is that α-KG acts as a substrate for 2-oxoglutarate-dependent dioxygenases (2-OGDDs) and activates Jumonji-C (JmjC) family lysine demethylases (KDMs), which belongs to 2-OGDD family and demethylates histone marks and regulate gene expression. As expected, the study revealed that BCAT1-mediated α-KG accumulation led to the downregulation of H3K27me3, a repressive histone mark associated with gene silencing. This demethylation, in turn, activated the transcription of glycolysis-related genes, enhancing glycolysis and promoting tumor progression.
The clinical relevance of BCAT1 in lung cancer was further explored using patient datasets and immunohistochemical staining. BCAT1 expression was significantly higher in primary lung adenocarcinoma (LUAD) tumors compared to normal lung tissues, and even higher in tumors from relapsed LUAD patients. Additionally, BCAT1 expression was significantly elevated in TKI-resistant NSCLC patients compared to TKI-sensitive patients, highlighting its potential as a biomarker for poor prognosis and TKI resistance.
To address the limited availability of effective BCAT1 inhibitors, the researchers developed and characterized WQQ-345, a novel BCAT1 inhibitor. WQQ-345 selectively inhibited the growth of BCAT1-highly expressing third-generation EGFR TKI-resistant cells in vitro and exhibited promising antitumor efficacy in resistant xenograft models. Mechanistically, WQQ-345 decreased cellular α-KG levels, upregulated H3K27me3 expression, and impaired glycolysis activity, further supporting the role of BCAT1 in mediating resistance to third-generation EGFR TKIs.
In conclusion, this study demonstrated the critical role of BCAT1 in mediating resistance to third-generation EGFR TKIs through epigenetic activation of glycolysis in NSCLC. BCAT1 facilitated BCAA anabolism and α-KG-dependent demethylation of H3K27me3, leading to the transcriptional activation of glycolysis-related genes, enhanced glycolysis, cell survival, and drug tolerance. The identification of WQQ-345 as a novel BCAT1 inhibitor further supports the therapeutic potential of targeting BCAT1 for the treatment of TKI-resistant NSCLC.
Reference:
Zhang T, Pan Z, Gao J, Wu Q, Bai G, Li Y, Tong L, Feng F, Lai M, Liu Y, Song P, Ning Y, Tang H, Luo W, Chen Y, Fang Y, Zhang H, Liu Q, Zhang Y, Wang H, Chen Z, Chen Y, Geng M, Ji H, Zhao G, Zhou H, Ding J, Xie H. Branched-chain amino acid transaminase 1 confers EGFR-TKI resistance through epigenetic glycolytic activation. Signal Transduct Target Ther. 2024 Aug 15;9(1):216.







Post comments