
by Dana-Farber Cancer Institute
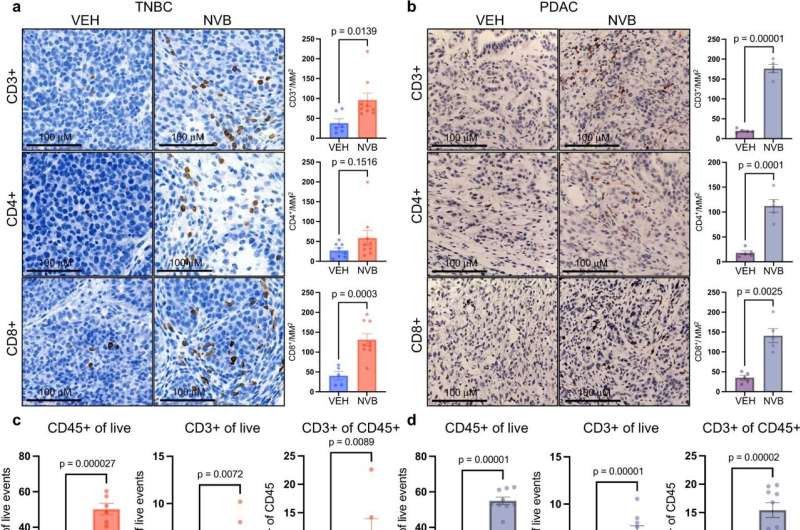
Efficacy of POLθ inhibition in HR-deficient cancers requires CD8+ T cells. a, b K14-Cre-Brca1f/f;Trp53f/f TNBC tumors from syngeneic FVB/129P2 mice (VEH, n = 5; NVB, n = 7) (a), or Brca2 KO KPC PDAC tumors from syngeneic C57BL/6 mice (VEH, n = 7; NVB, n = 6) (b) were subjected to IHC for CD3, CD4, and CD8 expression. Left: Representative IHC images at 40x magnification, scale bars, 100 μM. Right: Quantification of IHC using Aperio algorithms. Data, mean +/−SEM, unpaired two-tailed t-tests. c, d K14-Cre-Brca1f/f;Trp53f/f tumors TNBC (VEH, n = 7; NVB, n = 6) (c), or Brca2 KO KPC PDAC tumors (VEH, n = 10; NVB, n = 9) (d) were harvested 5 days after treatment and analyzed by flow cytometry. Scatter plots show significant increases in CD45+, CD3+, CD8+, and Granzyme B+ cells in NVB-treated animals. Error bars, SEM. Statistical analyses were performed using unpaired two-tailed t-tests. e, f TNBC tumors (VEH, n = 7; NVB, n = 6) (e) or PDAC tumors (VEH, n = 10; NVB, n = 9) (f) were analyzed by flow cytometry. Scatter plots show CD4+ cells, CD4+ T regulatory (FoxP3+) cells. Error bars, SEM. Statistical analyses were performed using unpaired two-tailed t-tests. g, h TNBC tumors (VEH, n = 7; NVB, n = 6) (g) or PDAC tumors (VEH, n = 10; NVB, n = 9) (h) were analyzed by flow cytometry for macrophages (CD11b + , CD11c-). Error bars, SEM. Statistical analyses were performed using unpaired two-tailed t-tests. i K14-Cre-Brca1f/f;Trp53f/f GEMM tumor-bearing syngeneic FVB/129P2 mice were treated with vehicle (n = 6) or NVB (75 mg/kg twice daily; n = 8), along with isotype control (n = 6) or an anti-CD8 antibody (200 µg twice weekly; n = 8) for 28 days. Graph shows the serial fold-change in tumor volume. Data, mean +/−SEM, one-way ANOVA analysis. j Brca2 KO KPC PDAC tumor-bearing syngeneic C57BL/6 mice were treated with vehicle (n = 9) or NVB (75 mg/kg twice daily; n = 10), along with isotype control (n = 9) or an anti-CD8 antibody (200 µg twice weekly; n = 10) for 28 days. Graph shows the serial fold-change in tumor volume. Data, mean +/−SEM, one-way ANOVA analysis. Credit: Nature Communications (2023). DOI: 10.1038/s41467-023-37096-6
As the first clinical trial of the drug novobiocin is about to open for patients with cancers carrying BRCA gene mutations, new research at Dana-Farber Cancer Institute shows the drug poses a double threat to tumor cells.
As reported today in Nature Communications, the researchers found that in addition to taking aim at the inner workings of BRCA-mutated cells, novobiocin also incites an immune system attack on the cells. The findings suggest that even if novobiocin proves as effective as hoped in clinical trials, it may work significantly better if paired with drugs that magnify the immune response.
In January, the U.S. Food and Drug Administration approved novobiocin for a clinical trial in patients with cancers harboring mutations in the BRCA1 or BRCA2 genes. The trial, to be led by Dana-Farber investigators, is expected to start enrolling patients by June 1.
"Novobiocin is an inhibitor of POLθ, an enzyme critical to the survival of cancers with mutations in BRCA1 or BRCA2," explains the study's lead author, Jeffrey Patterson-Fortin, MD, Ph.D., of Dana-Farber. "From previous research, we knew that disabling POLθ with novobiocin killed BRCA1- or BRCA2-mutant cancers. Here, we wanted to examine the contribution of the immune microenvironment—the immune system cells within a tumor—to the anticancer effect of novobiocin."
Using two tumor models—one of triple-negative breast cancer with BRCA1 mutations, and one of pancreatic cancer with BRCA2 mutations—researchers showed that novobiocin heightens the mayhem already occurring in cell division, with lethal consequences for tumor cells.
They found the drug causes tumor cells to become increasingly riddled with micronuclei—miniature nuclei that contain damaged fragments of chromosomes. The chromosome pieces slip easily through gaps in the micronuclei membranes and into the cells' cytoplasm, activating a protein pathway known as cGAS/STING. The pathway causes disease-fighting CD8+ T cells to invade the tumors and go into attack mode.
To determine the extent to which this process is responsible for the tumor cell-killing effect of novobiocin, Patterson-Fortin and his colleagues depleted CD8+ T cells from the two tumor models and found the effect of novobiocin was sharply diminished. "This demonstrates that the stimulation of the immune system is a major part of novobiocin's effectiveness, in addition to its direct effect on tumor cells," says the study's senior author, Geoffrey Shapiro, MD, Ph.D., of Dana-Farber.
One of the ways that the tumor cells adapt to the presence of novobiocin is by upping their production of the PD-L1 protein, which helps fend off a T-cell attack, Shapiro continues. This suggests that combining novobiocin with a PD-1-blocking agent could be more effective than novobiocin alone. Investigators hope to launch a clinical trial of the combination in the future.
More information: Jeffrey Patterson-Fortin et al, Polymerase θ inhibition activates the cGAS-STING pathway and cooperates with immune checkpoint blockade in models of BRCA-deficient cancer, Nature Communications (2023). DOI: 10.1038/s41467-023-37096-6. www.nature.com/articles/s41467-023-37096-6
Journal information: Nature Communications
Provided by Dana-Farber Cancer Institute






Post comments