
by Association of Basic Medical Sciences of FBIH
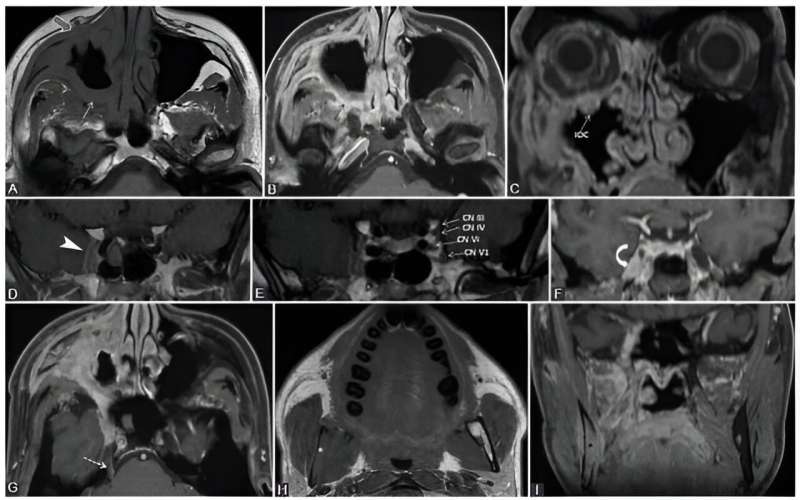
A. 39-year-old male diagnosed with adenoid cystic carcinoma of maxillary sinus, with multiple extensions. Clinically: Right abducens nerve palsy, diplopia, right infraorbital anesthesia. Axial T1-weighted (A, H), axial (B, G), and coronal (C, F, I) con-trast-enhanced (CE) 3D T1 FSPGR; coronal contrast enhanced in Phase T1 FSE IDEAL (D, E) images. The probable first point of PNS is PPF with fat obliteration (white arrow) and CE (black arrow), where the V2 nerve is involved. In an anterograde direction, the tumor reaches the right infraorbital nerve, demonstrated by infraorbital canal enlargement with CE (IOC) and preantral fat obliteration (gray arrow). Following the main V2 trunk, the tumor reaches the cavernous sinus which appears larger and shows CE (arrowhead). Note that in CN III, IV, V1, and V2 are situated in the lateral wall of the cavernous sinus, the cavernous segment of CN VI is located medially to the CN V1, implying the tumoral involvement of the mentioned nerves. There is Meckel's cave CE (curved arrow) and the tumor traveled back up to the main trigeminal trunk (cisternal segment, dashed arrow). Notice the right mandibu-lar fat replacement (white), associated with mandibular CE (black), and cortical disruption, meaning an anterograde PNS from the Meckel's cave to the inferior alveolar nerve (branch of V3). Credit: Bosnian Journal of Basic Medical Sciences
Peripheral neural spread (PNS) is a specific mode of cancerous invasion where tumor cells utilize nerves as pathways for local extension. This phenomenon is particularly significant in the realm of head and neck malignancies but can occur elsewhere in the body. The ability to accurately diagnose and understand PNS could revolutionize how we treat patients with head and neck cancers.
Researchers from Cluj-Napoca, Romania, have now provided an in-depth understanding of peripheral neural spread (PNS) in head and neck cancers, opening the door to better diagnostic and treatment approaches.
Head and neck cancers, affecting vital areas like the mouth, throat, and nose, are challenging due to their location and the intricate neural pathways in this region. When these cancers proliferate along nerves, they exhibit what's known as peripheral neural spread or more commonly, perineural spread (PNS). It's essentially the travel of cancer cells along the nerve pathways.
Cancer cells can spread either retrogradely (from the primary tumor towards the brain stem) or anterogradely (spreading to the periphery once the primary tumor reaches key connection points). Radiologists are cautioned to inspect the entire nerve as the spread might not be continuous.
Patients with PNS can present with a myriad symptoms, often misleading in their initial stages. These can range from numbness, tingling, or even pain in the regions served by the affected nerves. Some might experience facial weakness, difficulty swallowing, or altered sensations. Due to the subtle and varied presentation, a high index of suspicion is vital for early detection. Management may involve surgery to remove the tumor, radiation therapy to target the tumor cells, or a combination of both. The specific course of treatment depends on the extent of spread, the type of tumor, and its location.
Perineural invasion (PNI) describes the phenomenon where cancer cells invade the perineural space (the space surrounding the nerve). It's a pattern of invasion where tumor cells are actively infiltrating the nerve's protective layer. While PNI can be seen in various types of cancers, it's particularly prevalent in certain malignancies, including those of the head and neck, prostate, and skin (like cutaneous squamous cell carcinoma). Common manifestations include pain, often described as burning or shooting, numbness, and muscle weakness, with symptoms becoming more pronounced due to the invasion into the nerve itself. Histopathological examination, which involves looking at tissue samples under a microscope, is the gold standard for diagnosing PNI as it allows for visualization of the cancer cells within the nerve space.
PNI and PNS have a strong association with poor prognosis in head and neck cancers across almost all sites. This association extends to reduced local and regional disease control, increased risk of metastasis (both local and distant), recurrence, and reduced survival rates. The presence of PNI often indicates a more aggressive tumor behavior. This suggests a likelihood of the cancer recurring or metastasizing (spread to other parts of the body). Pain, which can vary in type and severity, is often described as deep-seated, burning, or shooting.
Potential issues with the accuracy and consistency of PNI reporting arise due to:
Variability in biopsy techniques.
Differences in detection methods.
Limited case studies.
Insufficient follow-up timeframes.
Lack of a universally accepted definition.
Using imaging to detect PNI/PNS poses challenges, as the literature displays inconsistencies and disagreements about its prognostic value.
The study by Romanian scientists found:
1. Phases of Muscular Denervation: Muscles, particularly those innervated by the mandibular nerve, undergo different phases when the nerves affecting them are compromised. These changes can be best seen on MRI scans, and understanding them can help distinguish between normal muscular changes and those caused by tumor invasion.
a. Acute (<1 month): Seen on MRI. It presents as T2 edema-like hypersignal and contrast enhancement (CE) in the affected muscle.
b. Subacute (up to 12-20 months): Observed on MRI. Characteristics include T2 prolongation, CE, no volume increase, or loss, and T1 hyperintensity due to fat transformation.
c. Chronic (after 12-20 months): Marked by fatty infiltration and neuropathic atrophy which can be seen on both CT and MRI.
2. SMAS Indicator: The superior musculoaponeurotic system (SMAS), a continuous fibrous network connecting facial muscles, has been identified as a potential indicator of PNS. PNS along CN VII branches can lead to the nodular thickening and enhancement of the SMAS structures. For those unfamiliar with the term, SMAS is essentially a fibrous network that connects facial muscles. Like an intricate web, it is continuous and underpins our facial structure. When changes occur within this system, particularly those visualized on imaging, it may hint at the presence of PNS. Recognizing such early signs can lead to timely interventions and better treatment outcomes.
3. Rare Indirect Findings: Signs like a small torus tubarius or mastoiditis can hint at Eustachian tube dysfunction, which might indicate V3 denervation. Obliteration of certain fat pads or chronic muscular denervation can suggest the presence of PNS. Noting such changes can guide doctors in optimizing imaging protocols for a more precise diagnosis.
4. There are vital nerve interconnections that cancer cells can exploit to spread. For instance, the greater superficial petrosal nerve and the auriculotemporal nerve are such interconnections.
5. Different studies have reported a range of findings regarding contrast enhancement in certain structures, such as the trigeminal ganglion. There are some inconsistencies in the literature regarding the extent and locations of enhancement.
6. Various other conditions, such as benign nerve tumors, neuritis, and radiation-induced neuropathy can mimic PNS.
Practical Implications for Patients and Clinicians
When a suspicious lesion is detected at crucial nerve intersections, all intersecting cranial nerves (CNs) should be thoroughly examined. Detailed knowledge of the regular MRI appearance of CNs is crucial. The Gasserian ganglion and its branches, for example, are usually avascular. Still, there are varying reports about contrast enhancements in these structures. With advancements in imaging technology, more precise visualization of CN pathology is anticipated. Techniques like MR neurography and CN tractography based on diffusion tensor imaging may offer more detailed insights into CNs, although current capabilities are still limited to thicker nerves or nerve groups.
Optimized Surgical Planning: Due to the unpredictable progression of PNS, experts now advise conducting imaging studies at least a month prior to surgery. This ensures that surgeons have the most recent and relevant information when planning their approach. The presence of PNI often prompts considerations for post-operative radiotherapy, especially in cases of resected skin and mucosal SCCa, aggressive salivary gland tumors, and any primary tumor showing clinical or radiological signs of PNS. Recognizing PNS is vital for pre-operative and radiation planning.
Enhanced Zonal Classification: Borrowing from the zonal classification system proposed by Williams et al., medical practitioners can now plan surgeries with better precision. This could lead to cleaner surgical margins and reduced complications.
Avoiding Misdiagnosis Pitfalls: The results highlight the need for precise imaging and an in-depth understanding of the condition. When doctors are aware of conditions and variations that could mimic PNS, they can make more accurate diagnoses.
Head and neck cancers, while accounting for approximately 4% of all cancers in the U.S., are particularly challenging due to their proximity to vital structures. The intricate nature of PNS only compounds this challenge. Understanding PNI/PNS is essential in the prognosis and management of head and neck cancers. Given the challenges in diagnosis, advancements in imaging techniques could prove invaluable. Adequate knowledge of cranial nerve anatomy and its typical and atypical presentations is crucial for healthcare professionals in this field.
More information: Olga Medvedev et al, Perineural spread in head and neck malignancies: imaging findings—an updated literature review, Bosnian Journal of Basic Medical Sciences (2021). DOI: 10.17305/bjbms.2021.5897
Provided by Association of Basic Medical Sciences of FBIH






Post comments