
by Annika Lund, Karolinska Institutet
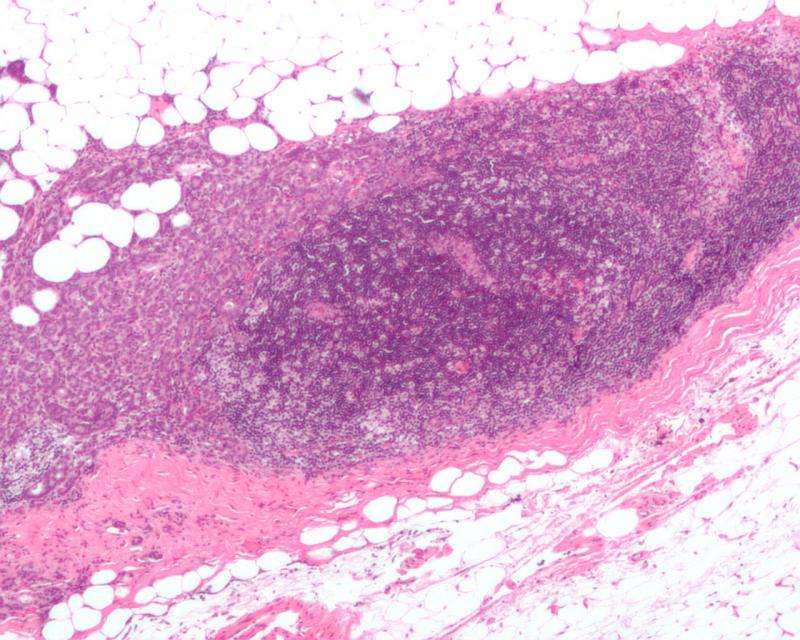
Micrograph showing a lymph node invaded by ductal breast carcinoma, with extension of the tumor beyond the lymph node. Credit: Nephron/Wikipedia
There is a lot going on within the field of breast cancer research. A new AI tool is trying to fine-tune the screening program, another one is helping pathologists make diagnoses. New drugs are approved. This could save more lives. But there is still no answer to the trickiest question of all: What causes breast cancer?
Breast cancer is a well-funded area of research. This is evident from a study published in The Lancet in 2023, in which researchers attempted to determine the actual distribution of a total of 24.5 billion dollars spent on cancer research at global level between 2016 and 2020. The single form of cancer that received the most money was breast cancer: 11.2% of the entire pot.
The abundant funding has had an impact. Mortality from breast cancer has fallen faster than mortality from other cancers. In 1980, 57.5% of patients survived at least 10 years with the disease. By 2022, the corresponding figure was 87.6%.
At the same time, the incidence curve shows an increase at all ages, most notably for women aged between 50 and 70. In 1980, 105 per 100,000 individuals were diagnosed with breast cancer in Sweden. By 2022, this figure had risen to 191 per 100,000. The increase is still ongoing and over the last two decades the number of cases has increased by about 2% per year.
More than 1 in 10 women over the age of 75 have been diagnosed with breast cancer, making it the most common cancer among women. In 2022, more than 8,500 people were diagnosed with breast cancer, including 57 men.
Thus, the disease is common and becoming more common, while survival rates are improving. Early detection, better diagnostics and more effective treatments are behind this success.
In Sweden, screening with mammography was gradually introduced starting in the 1980s. Today, all women between the ages of 40 and 74 are offered a free examination every 18 to 24 months.
Equal for all, in all regions. Very fair?
Absolutely not, says Per Hall, Professor at the Department of Medical Epidemiology and Biostatistics.
"Some women have a low risk of developing breast cancer while others have a very high risk. It is highly individual. We have had this knowledge for many years, but despite this we still screen everyone in the same way," he says.
New model for risk-based screening
Per Hall has spent the last decade developing a model for risk-based screening. With that goal in mind, an AI tool has had to work self-learning with mammography images from healthy women, images where it is known who later developed breast tumors. It may sound like a simple matter to enter a number of images into a system, but Per Hall describes a major challenge in making tens of thousands of images comparable even though they come from different digital environments, where different software has been used.
"It took several years to teach our software to treat all mammography images in the same way, whether the machine that took them was a Siemens or a Philips or any other brand," he says.
AI already has a place in the mammography business, with digital tools assessing the images. This way, radiologists can be relieved. In some mammography units, there is now one radiologist and AI looking at the images, instead of two radiologists as before. In those cases, the AI tool is tasked with answering the question "Are there any suspicious tumors in this breast?"
But the AI that Per Hall has been working on has learned something completely different. It is trained to answer the question "How likely is it that this breast will develop a breast cancer within two years?"
"The tool identifies and assesses a variety of parameters that the human eye cannot see. These include mammographic density in relation to age, calcifications and differences between the right and left breast," explains Per Hall.
Breast density is an important risk factor for breast cancer. Density is not something that can be seen or felt by the woman herself, but can be seen on a mammogram. A small amount of fat but a lot of breast tissue and connective tissue results in a dense breast. Conversely, a lot of fat and little other tissue results in a lower degree of density. In a dense breast with lots of breast tissue, there are more cells that can turn into cancer cells. It is also more difficult to see any tumors, as a dense breast will appear white on a mammogram, hiding any lump, which will also appear white on the image.
Risk factors affect the breast density
The density changes throughout life as breast tissue is converted to fat. In a 25-year-old, an almost completely white mammogram image is expected, but the same image from a 70-year-old woman would be a clear sign of a high risk of disease. Per Hall says that virtually all known risk factors for breast cancer affect density. Each child born and breastfeeding reduces density—so conversely, delayed childbirth, few children born and limited breastfeeding increases density. Alcohol and lack of physical activity increase density, as does post-menopausal obesity, late menopause or hormone therapy to relieve menopausal symptoms. The only known risk factors that reduce density are smoking and age.
"For some reason we don't know, smoking reduces the density while increasing the risk of breast cancer. But smoking is a risk factor—albeit a weak one—in this context," says Per Hall.
But many women have a lifestyle that includes the above-mentioned risk factors, without getting the disease. And some who get the disease are young, have given birth to several children early, drink sparingly and exercise frequently.
So many of the known risk factors for breast cancer are quite weak. But in a large group of women, as in a whole population, they make a difference. When an entire population changes its lifestyle in a certain direction, for example by postponing childbirth and having fewer children, this can partly explain why the disease is becoming more common.
A few known risk factors play a major role at the individual level. These include older age and, somewhat obviously, female gender. But also mutations in the BRCA1 and BRCA2 genes. They are rare, but they greatly increase the risk of developing the disease. Up to 5% of all breast cancer is caused by these mutations.
Per Hall believes that new knowledge about the genetics of breast cancer will eventually shed more light on the risk factors. He believes that certain gene variants, perhaps in combination with certain other gene variants, can amplify the effect of certain risk factors, leading to the development of the disease in an individual. But capturing that kind of combination of multiple factors, which are individually quite weak, in combination with one or more gene variants, requires enormously large studies to provide outcomes.
"We've collaborated with a large number of groups around the world and done studies involving about 400,000 women—but we're still not getting results. So we need even more participants to capture any patterns," says Per Hall.
It all boils down to the fact that it is currently impossible to say why a particular woman has developed breast cancer. Nevertheless, the researchers' goal is to be able to say approximately how likely it is that an individual woman will contract the disease within two years. And then renew the existing screening program from that perspective.
"Yes, exactly, that's what we are aiming for. We will test a possible approach in a study that starts now in April," says Per Hall.
The study he is talking about is called SMART and is part of the larger Karma project, which includes a large number of studies with different questions about breast cancer. In SMART, 70,000 women will be randomized into two groups. Half will be invited to join the existing screening program and offered screening at the current intervals. The rest will be risk assessed by the AI tool developed by Per Hall's research team. They will then be offered individually calculated intervals, where the high-risk women will be examined every year.
The high-risk women will also be examined in a different way, with a contrast agent injected via a vein in the arm before imaging. The agent seeks out any tumors that light up like little stars in the mammogram image, even whiter in all the white. The method is called contrast-enhanced mammography.
The hypothesis is that this will make it possible to find more breast cancers through screening. But—and this is tricky—not all breast cancers are equally important to find, as strange as that sounds.
A recurring criticism that has followed the mammography screening programs since their early days is that the more aggressive tumors slip through more easily. These tumors are more often detected when the woman herself feels a lump and therefore seeks care. Since this happens between the appointments in the screening program, it is called interval cancer.
Today, about two-thirds of breast tumors are detected through the screening program and about one in three breast cancers are interval cancers.
"It is the interval cancer that we want to address. We know that if you add more examinations to the screening program, you will find more tumors. But some of them can be considered as overdiagnosis. The important thing is to find cancers that would otherwise become interval cancers. This is how you manage to catch more cases of aggressive cancer at an earlier stage," says Per Hall.
The AI tool developed by his research team has recently been tested in a study with patients from four other European countries. The aim was to find out whether the tool also works in digital environments where it has not been trained. This resulted in a study recently published in The Lancet Regional Health.
The researchers included more than 8,500 women who all went home with good results from their mammograms. In that group, the researchers had "hidden" 739 women who were diagnosed with breast cancer within two years, before they attended their next screening appointment.
The question was: Does the AI tool find them? The answer is: Some.
In the large group of just over 8,500 women, the tool has deemed just over 529 to be at "high risk" of getting an interval cancer. And in this smaller group, nearly one in three women did indeed get it. And of those, about one in three had disease that had grown slightly larger or spread to lymph nodes in the armpit.
"The tool succeeded in detecting both interval cancer and more aggressive cancer. And with a method that is not particularly expensive—we don't do any genetic analysis or MRI scans," says Per Hall.
In the best case, a trimmed screening program can contribute to more tumors being found early. But once they are caught, accurate diagnosis is crucial for the patient to get the best possible treatment. And AI has an important role to play here too.
"AI is at its best when it comes to seeing patterns in images. The use of AI in pathology will be of great importance and is a journey that has only just begun," says Johan Hartman, Professor of Tumor Pathology at the Department of Oncology-Pathology at Karolinska Institutet.
He describes a rapid pace of development, with digitalization still ongoing. Many hospitals have put away the microscopes and are fully digital. In other places, the transition is still ongoing. In parallel, the next stage of development is already taking place, supported by AI.
More specifically, digital pathology means that a tissue sample is first handled manually, just like before. For example, a specimen may be thinly sliced and placed on a glass slide. It is then sent into a scanner that can photograph hundreds of slides at a time.
It is these extreme close-ups of the tumors that pathologists analyze. In many cases, this involves counting, assessing and evaluating. For example, a certain percentage of cells must have receptors for estrogen and progesterone for a tumor to be considered hormone sensitive. The proportion of cells in the division phase describes the growth rate. There are other aspects that are important for categorizing a tumor.
"But we are only human. It is difficult to quantify different things in an image," says Johan Hartman.
At least for a human. An AI can count every cell in an image and assess it—at lightning speed.
"These systems, where AI helps us count, already exist today. I think they will soon become a requirement in pathology," he says.
A number of parameters
Johan Hartmans research focuses on the next generation of AI—a more analytical model, capable of assessing the severity of disease in the cells on the screen.
"That's the type of AI I'm most interested in. These are systems that will have a major impact on diagnostics," says Johan Hartman.
He and his colleagues have developed an AI tool that is already being used to assess hormone-sensitive breast cancer, which accounts for about 80 of cases. This large group is divided into lots of different subgroups, in different ways.
The concept of tumor grade is relevant in this context. This assessment is based on a number of parameters. For example, in addition to growth rate, the pathologist must estimate how abnormal the cells are, in general—what do the cell nuclei look like, how much do they differ from healthy cell nuclei? And are the cancer cells similar or different from each other?
"A human is capable of holding a maximum of ten variables in his or her head and weighing them together in an overall analysis. This AI system is capable of assessing and weighing thousands of variables," says Johan Hartman.
Today, breast tumors are divided into three groups, where tumor grade 1 means a low risk of recurrence and spread, while tumor grade 3 is associated with higher risks.
But in practice, more than half of the tumors fall into an intermediate group, grade 2. This means thousands of cases per year. And for them, the choice of treatment is less obvious.
"Oncologists often choose the safe option and add chemotherapy and radiation in many cases. This means that there are patients in this intermediate group who are overtreated," says Johan Hartman.
The AI he has developed has accessed thousands of images representing grade 1 and 3 tumors. The tool has had to work self-learning in this large image material and train itself in pattern recognition. The goal was to figure out what separates the two groups.
And the system has succeeded in doing so. When the tool assesses images from the large intermediate group, it manages to place the tumors along a scale, with some closer to grade 1 and others closer to grade 3. In studies where the researchers have known which patients who have later relapsed, it has been shown that the tool makes good assessments.
Some hospitals in the country have already started using the AI tool to support them.
"The tool contributes to a more uniform assessment of the tumor. We know today that assessments can vary depending on the pathologist who makes them. This is a problem because it can affect treatment choices. This tool contributes to a common understanding of tumor categorization, regardless of where in the country the patient is treated," says Johan Hartman.
Over the last decade, a number of new drugs have been developed in the field of breast cancer, such as CDK4/6 inhibitors, which can slow down hormone-sensitive disease that has spread beyond the breast and armpit. There have also been several new immune therapies that help the body's own immune system fight the tumors. There are more new treatments in addition to these, including several that improve the effectiveness of the anti-hormonal treatments used for hormone-sensitive cancer.
Theodoros Foukakis, an oncologist and research group leader at the Department of Oncology-Pathology at Karolinska Institutet, is investigating how to tune different drug treatments in the clinical situation. The aim is to give doctors better opportunities to make wise choices for each patient—as effectively as possible, with as few side effects as possible. Everything is investigated with classic clinical trials, where patients are randomized between different treatment options and followed over time. Many of the studies are conducted in large international collaborations.
Promising immunotherapy
A specific example is studies on the immunotherapy Keytruda, with the active substance pembrolizumab. This drug was previously given in the breast cancer field only to women with metastatic triple-negative breast cancer, where the disease has sent distant metastases to, for example, the bones, lungs or liver. Disseminated breast cancer is currently incurable, so the aim is to slow down the disease and prolong life.
Triple-negative breast cancer means that the cells lack receptors for estrogen, progesterone and HER2. Because many treatments are designed to block these receptors, there are fewer drugs available for triple-negative breast cancer, which is often more aggressive and in many cases affects younger women.
In triple-negative breast cancer, treatment usually starts with chemotherapy to shrink the tumor before surgery. Theodoros Foukakis has led the Swedish part of a study that has tested a new approach to the treatment given before surgery. In this study, women were randomized into two groups: half received chemotherapy with the addition of the immunotherapy pembrolizumab, and the rest received chemotherapy and a placebo. After surgery, the women continued treatment with either immunotherapy or placebo.
Five years later, nearly 19 of those who received additional immunotherapy had relapsed. The corresponding figure for those who only received chemotherapy was 28. A difference of 9 percentage points. And most of the relapses were not a new tumor in the breast, but spread disease with distant metastases.
Roughly speaking, just under a thousand women per year are diagnosed with triple-negative breast cancer in Sweden. This means that just under a hundred women avoid relapse if immunotherapy is included in the treatment given before surgery. This treatment approach is now clinical practice in Sweden for this patient group.
"That 9% is very important. Many of those who relapse cannot be cured," says Theodoros Foukakis.
Another part of his research involves finding biomarkers in patients. Again, the goal is to understand who benefits from a particular treatment.
"This is research that pharmaceutical companies are not always interested in doing. But in the clinic, we need to be able to identify the different subgroups that will or will not benefit from different drugs so that we can make the right choice. Otherwise, patients risk receiving drugs that do not help them but only cause side effects, says Theodoros Foukakis.
Journal information: The Lancet
Provided by Karolinska Institutet





Post comments