
by Gillian Rutherford, University of Alberta

Credit: University of Alberta
A University of Alberta team has developed a device to provide a more reliable, aseptic and economical treatment for frostbite, to be used in emergency rooms, shelters and even outdoors.
"Frostbite disproportionately affects opioid users, unhoused persons, people with mental illness and socially isolated people," says Matthew Douma, RN, adjunct professor of critical care medicine in the Faculty of Medicine & Dentistry and co-principal investigator of a project looking into frostbite cases in Alberta. "This is a condition that has been inadequately treated due to neglect and marginalization."
The device, known as a Precision Warm Water Circulator, is inspired by the sous vide cooking method, because it provides continuously circulating water at a precise temperature, in the case of the device between 37°C and 42°C. The device is portable, operated from a cart and can be supplied with a battery pack. The water basin is 20 centimeters deep.
"Evidence reviews show that the best possible treatment for frostbite is immediate or rapid immersion in circulating warm water," says Douma, who helps write treatment guidelines for the American Red Cross, the American Heart Association and the Heart and Stroke Foundation of Canada.
Douma says his team considered the alternatives and came up with the device as the solution to all of the other methods' problems: A tub of warm water cools too quickly. Running water from a tap is not always a consistent temperature, risking burns to the skin, and sinks are not sanitary. Tucking frozen hands under your arms—which you may have learned as a child—might warm hands that are cold but does not provide enough heat to remedy frostbite.
Exposed skin starts to freeze at 0°C. At first it starts to feel more firm to the touch, and will eventually freeze solid. The freezing process is usually painful though, dangerously, the pain disappears once the skin and its nerves are completely frozen. Damage to blood vessels and cells is caused by ice crystals in the tissue that interfere with circulation, ultimately leading to tissue death. Frozen tissue will turn black about three days after the injury.
Douma and his co-principal investigator Scott MacLean, assistant professor of emergency medicine at the U of A and physician at Edmonton's Royal Alexandra Hospital, reviewed Alberta hospital records over the past three years to track frostbite diagnoses.
They found more than 1,500 cases of frostbite per year across the province, including more than 100 each year that were serious enough to require amputation.
That's why Douma is making the device available through a non-profit social enterprise called Miteh Health Solutions at the cost-recovery price of about $7,000 per unit, with a "buy one, give one" model where devices purchased result in a device being donated to charities and not-for-profit organizations, like emergency shelters.
"I realized there's a big gap between what ought to be done and what is actually done," explains Douma. "I wanted to do something this year, for this frostbite season, to make it easier for people who work in emergency departments and shelters to rewarm frostbite and prevent a lifetime of disability for patients."
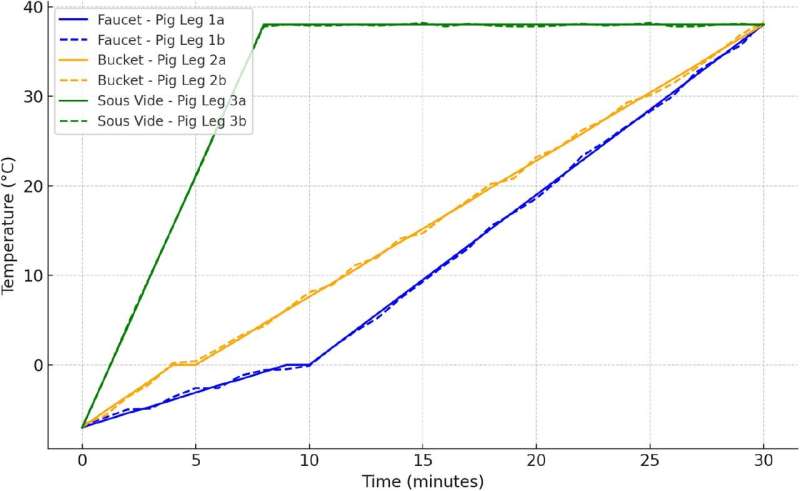
Time to reach target tissue temperature for faucet/sink, bucket, and immersion circulator (sous vide) methods. Credit: medRxiv (2024). DOI: 10.1101/2024.11.04.24316457
The device has gone through preclinical testing using frozen pig legs and healthy volunteers, and it outperformed two other rewarming methods—using a bucket of water and using a sink and faucet—according to the team. The research article is posted to the medRxiv preprint server.
"Our study concludes that the immersion circulator method is superior to other methods as it achieves faster and more consistent rewarming," they report. "This method has the potential to enhance frostbite treatment protocols, particularly in clinical and field settings where consistent rewarming is difficult to achieve."
Douma notes that time is of the essence when it comes to saving tissue.
"The science around frostbite and rewarming is not as robust as, say, the science around heart attack or stroke, but we think the same concepts apply and that it's a time-sensitive condition," he says. "While tissue is frozen, it isn't getting blood flow. So the tissue is dying. We need to rapidly get the blood flow back just like you do for a heart attack or stroke."
Frostbite occurs in four categories, with grade four always leading to tissue loss. Douma believes with aggressive frostbite screening and timely rewarming, more limbs and digits can be saved, and other treatments can be introduced, including a medication called iloprost, a still-experimental vasodilator that allows blood vessels to relax and increases blood flow.
"We need to aggressively rewarm and see if patients are candidates for intravenous medication therapy," Douma says.
To determine iloprost's efficacy, Douma and MacLean have been comparing outcomes between frostbite cases in Edmonton, where iloprost is not typically administered, with similar cases in Calgary that did use the medication. The team plans to share the results with the City of Calgary, City of Edmonton and social services agencies such as Homeward Trust.
More information: Matthew J. Douma and Jaskirat D. Tiwana, Frostbite Immersion Rewarming Methods: Sink & Faucet vs Bucket vs Immersion Circulator, medRxiv (2024). DOI: 10.1101/2024.11.04.24316457
Journal information: medRxiv
Provided by University of Alberta







Post comments