
byJustin Jackson, Medical Xpress
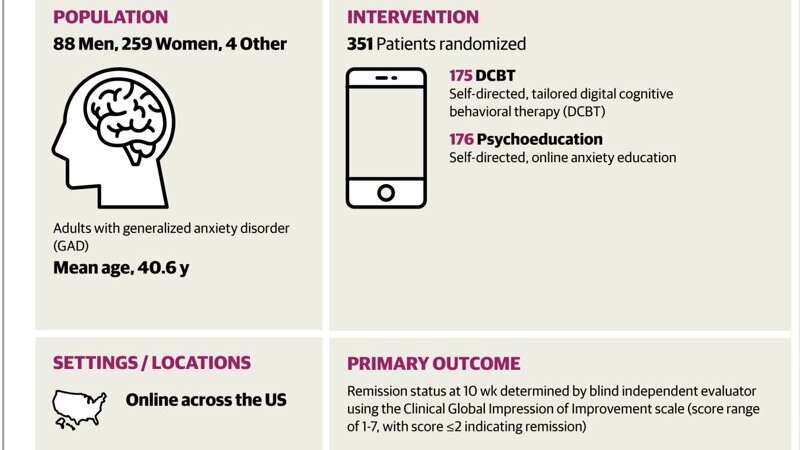
Visual abstract. Credit:JAMA Network Open(2025). DOI: 10.1001/jamanetworkopen.2025.48884
Big Health Inc, along with paid academic investigators, reports higher remission rates and lower anxiety symptom scores with their smartphone-delivered digital cognitive behavioral therapy, DaylightRx, compared with an online psychoeducation, also created by Big Health Inc.
Generalized anxiety disorder involves excessive, persistent, and uncontrollable anxiety with lifetime prevalence reported as 6%, alongside reduced quality of life, impaired social and occupational functioning, and increased health care utilization.
Cognitive behavioral therapy and pharmacotherapy are considered first-line treatments. Despite strong tolerability, efficacy, and cost-effectiveness, access remains limited due to a shortage of trained therapists, time burdens, and stigma.
Digital deliveryhas been proposed to address access barriers by expanding reach. Smartphones offer real-time access and near-universal availability. Meta-analytic reviews of early smartphone interventions for anxiety suggest limited effectiveness, prompting interest in more structured digital applications that incorporate core elements of cognitive behavioral therapy.
DaylightRx delivers audio-guided exercises and interactive instruction in cognitive restructuring, applied relaxation, stimulus control, avoidance reduction, mindfulness, problem solving, and imaginal exposure. All content is accessed via smartphone, with tools designed for everyday use through regular engagement.
In the study, "Digital Cognitive Behavioral Treatment for Generalized Anxiety Disorder," published inJAMA Network Open, researchers tested a smartphone-based therapy called DaylightRx against a psychoeducation control in adults diagnosed with generalized anxiety disorder.
Trial procedures were fully remote and coordinated by Boston University. The cohort included 351 participants with generalized anxiety disorder confirmed by a structured interview, and scores of 15 or higher on the 7-item Generalized Anxiety Disorder scale. Screened-out conditions covered moderate or greater suicide risk, bipolar disorder, psychosis, obsessive compulsive disorder, and recent substance use disorder.
Control participants received written online psychoeducation covering symptoms, prevalence, causes, consequences, and lifestyle advice, with self-paced access and encouragement to apply material.
Since the psychoeducation control was created by Big Health Inc, the sponsor of the study and the creator of DaylightRx (the intervention the control is meant to gauge the effectiveness of), any result would only apply to this specific scenario and should not be generalized.
Clinical Global Impressions–Improvement (CGI-I) scale and self-reported anxiety severity with the 7-item Generalized Anxiety Disorder (GAD) scale, assessed at 10 weeks and 24 weeks after randomization. "Remission" used a Clinical Global Impressions–Improvement score of 2 or lower. Primary outcomes used blinded independent evaluator ratings for "remission."
Remission is in quotes for this article, though it was not in the study, as this term was redefined internally by the study design. Remission typically refers to a state of minimal or absent symptoms, sustained over time, and often confirmed via structured diagnostic reassessment.
"Remission" is used in two distinct ways across the trial without consistent distinction. The primary outcome defines remission using a CGI-I score ≤ 2, based on evaluator judgment of improvement. A secondary outcome defines remission as a GAD-7 score <10 at week six, a self-reported symptom cutoff. Neither definition involves clinical reassessment or functional recovery metrics.
This dual use creates terminological ambiguity and may inflate the clinical impression of symptom change, particularly where "remission" might imply a diagnostic resolution.
Operational meaning differs by context within the report, and makes the use of "remission" more of a result of a branding effort that borders on misleading lay readers into believing the treatment is far more effective than evidenced by the study.
"Remission" at 10 weeks occurred in 71.0% of DaylightRx digital cognitive behavioral therapy participants with video visit data, compared with 34.6% of Big Health psychoeducation participants. "Remission" at 24 weeks occurred in 77.7% of digital cognitive behavioral therapy participants with video visit data, compared with 52.0% of their psychoeducation participants.
The mean 7-item Generalized Anxiety Disorder scale score at 10 weeks was 7.88 for digital cognitive behavioral therapy and 11.68 for psychoeducation. The mean score at 24 weeks was 7.23 for digital cognitive behavioral therapy and 10.68 for psychoeducation.
Events potentially related to digital cognitive behavioral therapy use included panic attacks at 2.9%, depression symptoms at 2.9%, hormonal or seasonal mood symptoms at 1.7%, suicidal ideation at 1.7%, posttraumatic stress disorder symptoms at 0.6%, musculoskeletal pain at 3.4%, and headache at 1.7%.
A number of unintended unblinding events occurred, all in the digital cognitive behavioral therapy arm, with sensitivity analyses described as robust when excluding those participants. Numerical results of the sensitivity analyses, or how the authors defined "robust," were also excluded.
Researchers concluded that smartphone-delivered digital cognitive behavioral therapy offered significant and sustained benefits to adults with generalized anxiety disorder, with advantages over self-directed online psychoeducation at 10 weeks and 24 weeks.
Validation of a digital cognitive behavioral therapy program intended for prescribing by mental health and primary care practitioners would require a trial against established criteria and efficacy would need comparisons to existing validated methods, none of which occurred in the current study, leaving any unbiased conclusions unclear.
Use of "remission" as a clinical-sounding endpoint creates the appearance of psychiatric resolution, which may not be warranted by a drop in score alone. Readers unfamiliar with measurement-based care may misinterpret this as diagnostic remission, rather than symptom score reduction.
© 2025 Science X Network
More information E. Marie Parsons et al, Digital Cognitive Behavioral Treatment for Generalized Anxiety Disorder, JAMA Network Open (2025). DOI: 10.1001/jamanetworkopen.2025.48884 Journal information: JAMA Network Open





Post comments