
By Brett Sears, PT
Medically reviewed by David Strosberg, MD
Anterior cervical discectomy and fusion (ACDF) is a type of spine surgery used for the treatment of neck or arm pain caused by cervical radiculopathy. This surgery involves the removal of a protruding disc from the spine for relief of pressure on the spinal nerves, followed by reconstruction.
It can take several weeks or months to recover after surgery, and most people experience significant relief of symptoms after healing.1 However, you might have persistent neck pain or a permanent decrease in your neck mobility, and there is a risk of complications, including nerve damage.
Verywell / JR Bee
What Is ACDF?
Your spine (backbone) is a column of individual vertebral bones separated by cartilaginous discs and stabilized by muscles, ligaments, and tendons. The spine protects the spinal cord and spinal nerves, which control movement and sensation. Your cervical spine, located in your neck, is the upper part of your spine.
An ACDF is a complex spine procedure that may involve each of these structures. It is done by a spine surgeon, who can be an orthopedic surgeon or a neurosurgeon.
While an incision in the front of the neck (anterior approach) is typical for ACDF, this may not be possible if you have a structural issue in that location that could interfere with surgery. In this case, if your healthcare provider believes that you would benefit from cervical discectomy and fusion, you might have the surgery with a posterior (back of the neck) approach.2
The procedure is done under general anesthesia and involves several elements:
Removal of the disc that's causing your pain or weakness (discectomy)
Stabilization of the adjacent vertebrae
Placement of a graft in the space that had been occupied by the disc
Positioning of surgical hardware for cervical fusion3
The bones heal together, resulting in permanent fusion. The fusion may limit the range of motion of your neck.
You might have a more extensive or complicated surgery if you have multiple levels of disease or if you have bone deformities in addition to disc impingement.
Contraindications
Not everyone is a candidate for an ACDF. Your healthcare provider will discuss the risks and benefits of this procedure with you as you consider treatment options for your neck pain.
Contraindications include systemic disease and spine disease:
If you have a debilitating illness that could inhibit your ability to participate in physical therapy during recovery, you might develop substantially impaired mobility after having this surgery.
A movement disorder or weakness from a stroke can make it difficult for you to adjust to the effects of bone fusion during and after the healing process.
Severe spine deformities can interfere with this procedure, potentially making proper positioning for spine fusion impossible.
A bone disorder such as osteoporosis can impair bone healing, with inadequate fusion after surgery.
Risks
There are inherent risks with spine surgery and anesthesia. An ACDF is a major surgical procedure that can cause serious physical impairment if there is damage to any of the structures involved.
Specific risks of ACDF surgery include:4
Persistence or worsening of symptoms
Mild weakness or sensory disturbance in one or both arms and/or legs
Difficulty swallowing food or water
Impaired speech
Paralysis of one or both arms and/or legs
Loss of bowel or bladder control
Death
While possible complications are quite serious, the risk of post-operative problems is low. Surgery is generally successful, usually resulting in an improvement in symptoms.4
Purpose of ACDF
An ACDF is done to relieve cervical radiculopathy, which is pressure on a cervical spinal nerve. Degeneration, trauma, or disease of a vertebral disc can lead to disc herniation (movement from its normal space) and can cause impingement on the spine or spinal nerves.
A disc that's impinging on these structures may need to be removed because it's usually not repairable.
Symptoms can occur suddenly or may develop slowly over time. Those that may be relieved with ACDF include:
Neck pain
Decreased range of motion of your neck
Pain in your arm or hand
Numbness or tingling in your arm or hand
Weakness in your arm or hand
Diminished coordination of your hand or arm
You might be taking large amounts of pain medication for relief, and surgery can help you reduce that.
A shorter duration of symptoms and severe pre-operative weakness and/or pain is associated with more significant improvement after ACDF surgery than mild weakness or chronic symptoms.5
However, it's important to know that neck and arm pain caused by cervical radiculopathy might not improve with any type of surgery—including ACDF.
Generally, conservative management is recommended before surgery is considered—even if you have cervical radiculopathy caused by a disc pressure. This may include:
Oral pain or anti-inflammatory medication
Physical therapy
Massage therapy
Spinal injections
If you don't experience adequate improvement from non-surgical management, your healthcare provider may suggest that you consider ACDF surgery.
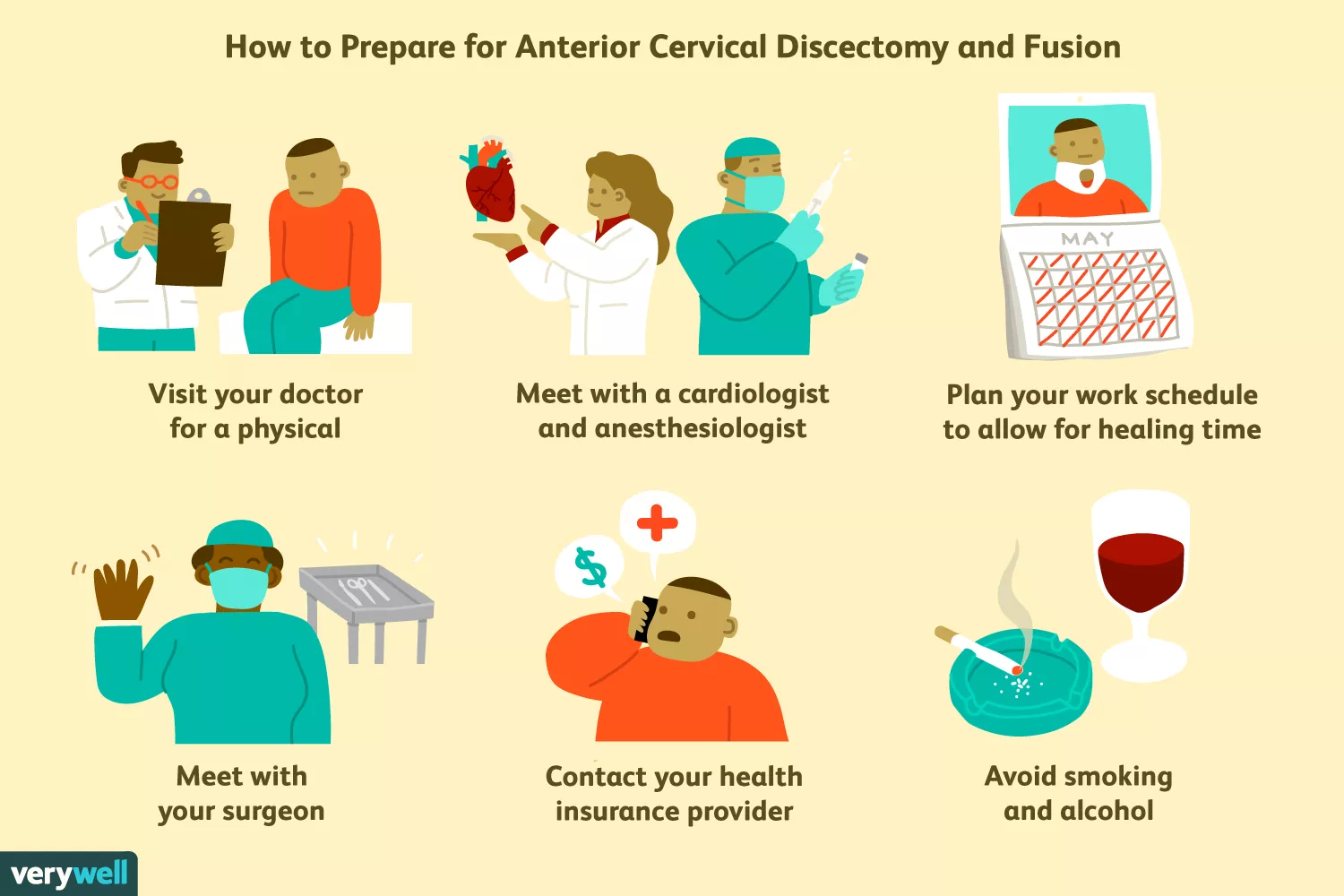
How to Prepare
ACDF surgery outcomes can differ, and treatment plans need to be tailored to each individual case. You and your healthcare provider will have a discussion about the likelihood of improvement based on your symptoms, the duration of your condition, and the anatomical issues seen on your imaging studies.
Before deciding if and when to have your ACDF procedure, you will need to ensure that you can take time for the recovery, which includes several days of rest, several weeks or months weeks of limited activity of your neck and arms, and months of physical therapy.
Prior to your surgery, you will have a thorough physical examination and diagnostic tests to determine the location and structure of your spine problem. You can also discuss the size and location of the surgical scar with your healthcare provider.
Additionally, you will need to have pre-operative testing for your general anesthesia planning. Your pre-operative testing will include an electrocardiogram (EKG), a chest X-ray, and blood tests, including a complete blood count (CBC) and blood chemistry levels.
Location
Your surgery will be done in a surgical operating room in a hospital or surgical center.
What to Wear
Wear something comfortable when you arrive for your surgery appointment. You will need to wear a hospital gown during your procedure. Make sure whatever you plan to wear home is loose around the neck.
Food and Drink
You need to fast (no food or drink) after midnight the night before your surgery.
Medications
Your healthcare provider will advise you regarding medication adjustments before your surgery. You will likely need to discontinue or decrease any blood thinners or anti-inflammatory medications that you regularly take for several days prior to surgery.
You may need to adjust your dose of diabetes or steroid medications in the days before your surgery as well.
What to Bring
Be sure to bring a form of identification, your health insurance information, and a method of payment.
You will need to have someone with you who can drive you home after your surgery.
Pre-Op Lifestyle Changes
Your healthcare provider or physical therapist will let you know if you need to adjust your neck movements or wear a neck brace to avoid further injuries prior to your surgery.
What to Expect on the Day of Surgery
When you go in for your surgery, you will have to register and sign a consent form.
You will go to a pre-operative area and change into a hospital gown. Your nurse will check your temperature, pulse, blood pressure, and oxygen level and place an intravenous (IV, in a vein) line in your hand or arm.
Possible same-day tests include:
Imaging of your cervical spine
Blood tests, including a CBC and chemistry panel
Your medical team will want to ensure that you don't have an acute illness before proceeding with your surgery. If you have a severe infection or another major medical issue, you may need to have your surgery postponed until the medical issue improves.
You will meet with your surgeon and anesthesiologist. Your surgeon may re-check your strength and sensation to see if there are any changes before your surgery.
Before the Surgery
Your anesthesia and surgical preparation will begin in the operating room. You will have general anesthesia, so you won't be able to feel anything. You will be sleeping and unable to move during this surgery.
During your surgery, you may have a urinary catheter in place, and this would most likely be placed as your surgical and anesthesia team members are getting you ready for surgery in the operating room.
Anesthesia monitoring devices will be placed to measure your oxygen saturation, pulse, respiratory rate, and blood pressure throughout your procedure. Anesthetic medication will be injected into your IV to make you sleepy and to paralyze your muscles.
A breathing tube will be inserted into your airway so you can have mechanical breathing assistance throughout your procedure.
You will be positioned so your surgeon can perform your surgery. Your surgical team will place a drape over your body, exposing the area on your neck where you will have your surgical incision. Your skin will be cleaned with antiseptic.
During the Surgery
Your surgeon will begin by making an incision at the front of your neck to one side of your windpipe (unless otherwise planned). As your surgeon gently cuts deeper, your windpipe and food tube will be carefully moved aside.2
The front of your cervical spine will be located. Care will be taken to ensure your spinal cord, nerves, and spinal blood vessels are not disturbed during this procedure.6
Then, each element of the ACDF will be performed in order:3
One or more ligaments may need to be partially cut for access to remove the damaged disc material.
Your pain-inducing vertebral disc will be removed.
If you have bony arthritis or scar tissue that's causing nerve impingement, it will be cut away.
A small metal spacer will be inserted between the vertebrae where your disc had been.
If you are having an autograft, a small piece of your own bone will likely be taken from your hip. Your surgeon will access your bone through a skin incision; sutures, a bandage, and gauze will be placed on the area from which the bone is harvested.
A compound will be used to fill in the space between the vertebral bones. This compound is mixed with small parts of your own bone (autograft) or with donor bone cells (allograft). The compound will help fuse the two vertebrae together.
A small metal plate will be attached to the front of the two vertebrae using tiny screws. This permanent plate helps hold the bones in place while you heal.
When the discectomy and graft placement are complete, your food tube and windpipe are returned to their anatomical positions, and any tissue that needs to be repaired (such as a ligament that was cut) is addressed with sutures. Your skin will be closed with sutures and your neck will be covered with bandages and gauze.
Your anesthesia medication will be stopped and your breathing tube will be removed so you can begin to breathe on your own. Once your ACDF surgery is complete and you are stable, you will go to the recovery area.
After the Surgery
In the post-operative recovery area, you will continue to have your oxygen saturation, pulse, blood pressure, and respiratory rate monitored for a few hours. You will likely be groggy. Your medical team will check on your pain and give you pain medications as needed.
If you had a urinary catheter during your surgery, it will be removed in the post-operative area and you may be asked to get up (with assistance) to use the toilet after the catheter is removed.
Your healthcare provider will meet with you to discuss how the procedure went. You will have a physical examination to check your sensation and your reflexes, as well as your strength. Don't worry if it's hard for you to move—any effort you make will be enough to give your practitioner a sense of your muscle strength.
You might be discharged on the same day of your procedure or stay in the hospital overnight.7
Your healthcare provider may instruct you to wear a soft cervical collar or a neck brace. If that's the case, your medical team will show you how to put it on and take it off, and give you instructions regarding when you should wear it and for how long.
Before you go home, you will receive instructions about pain medications, activity, exercise, complications to look out for, and when to make your follow-up appointments. You should also get instructions about how to resume any medications that were adjusted prior to your surgery, such as blood thinners or diabetes medications.
Recovery
Recovery from ACDF surgery takes about six to eight weeks. Your course of healing may be slightly shorter or longer depending on your overall health, the severity of your cervical spine disease, and the extent of your surgery.
Throughout your recovery period, you will have several follow-up appointments with your surgeon, neck imaging studies to assess your healing, removal of sutures, and physical therapy.
Activity
You will need to take it easy for several days. Follow instructions when it comes to neck support, advancing your neck motion, moving your arms, and so on.
Things to avoid in the first few weeks after surgery include:
Heavy lifting
Sexual intercourse
Excessive bending or rotating of your neck
Swimming
Driving
You should avoid strenuous activities for about four to six weeks after ACDF surgery.
Most people benefit from gentle exercise after ACDF surgery; you will be permitted and encouraged to walk. Starting a walking program can help you improve your endurance and fitness while getting back to your normal lifestyle.
Your physical therapy may begin within a few weeks of ACDF surgery. Your therapist can assess your condition and prescribe exercises that can help you regain neck mobility, strength, and postural control.
Healing
Instructions regarding bathing and keeping your incision clean and dry will depend on the type of sutures and wound dressing that you have.
You will be able to take pain medications as prescribed, but it's important that you avoid pain medications that could cause bleeding or interfere with healing, including over-the-counter anti-inflammatories.
Narcotic pain medications can cause constipation, so your medical team will give you instructions regarding medications or dietary modifications to manage this side effect if you will be using this type of pain control.
If you are in doubt as to what your medical team would consider normal during the healing process (e.g., level of discomfort, swelling), don't hesitate to call your healthcare provider's office. Complications can lead to serious permanent issues, like loss of arm and/or leg function.
Signs of postoperative complications include:
Fever
Bleeding or pus from your incision
Swelling and redness around your incision
Hoarseness of your voice that does not improve within a few days of surgery
Difficulty swallowing
Severe and persistent headache
Arm pain or paresthesia (unpleasant or unusual sensations) that does not improve within a few days of surgery
Weakness or paralysis or your arm, hand, foot, or leg
Decreased bowel or bladder control
Severe pain or discomfort when advancing physical activity as directed
Be sure to call your healthcare provider right away if you experience any of these issues.
Coping With Recovery
You will not be able to drive and you may need assistance with your routine self-care (such as getting dressed) for several weeks or months after your surgery.
Be sure to follow the individualized instructions that are given to you by your surgeon or physical therapist, including those related to going back to work.
Long-Term Care
After you have fully healed, you should be able to participate in a greater variety of physical activity. You might have limited motion of your neck, and your physical therapist should be able to guide you on how to adapt to any new limitations resulting from your surgery.
Possible Future Surgeries
While many people experience relief from pain after this surgery, approximately 26% of people who have had ACDF subsequently experience cervical radiculopathy in an adjacent disc.1
In some cases, the fusion site between the vertebrae doesn't heal properly (pseudoarthrosis). Surgery may need to be repeated.4
Lifestyle Adjustments
Overall, it is important that you seek guidance so you can learn how to avoid further injuring your neck.
For instance, it is a good idea to avoiding sitting in a hunched position for prolonged periods of time or lifting heavy objects without following guidelines for neck safety.
Your physical therapist should be able to point you in the right direction when it comes to optimal positions for your neck.
Sources
O'Neill KR, Wilson RJ, Burns KM, et al. Anterior cervical discectomy and fusion for adjacent segment disease: Clinical outcomes and cost utility of surgical intervention. Clin Spine Surg. 2016;29(6):234-41. doi:10.1097/BSD.0b013e31828ffc54
Audat ZA, Fawareh MD, Radydeh AM, et al. Anterior versus posterior approach to treat cervical spondylotic myelopathy, clinical and radiological results with long period of follow-up. SAGE Open Med. 2018;6:2050312118766199. doi:10.1177/2050312118766199
Rhee JM, Ju KL. Anterior cervical discectomy and fusion. JBJS Essent Surg Tech. 2016;6(4):e37. doi:10.2106/JBJS.ST.15.00056
Epstein NE. A review of complication rates for anterior cervical diskectomy and fusion (ACDF). Surg Neurol Int. 2019;10:100. doi:10.25259/SNI-191-2019
Shenoy K, Patel PD, Henstenburg JM, et al. Impact of Preoperative Weakness and Duration of Symptoms on Health-Related Quality-of-Life Outcomes Following Anterior Cervical Discectomy and Fusion. Spine J. 2020;S1529-9430(20)30822-6. doi:10.1016/j.spinee.2020.06.016
Mohandas A, Summa C, Worthington WB, et al. Best Practices for Outpatient Anterior Cervical Surgery: Results From a Delphi Panel. Spine (Phila Pa 1976). 2017;42(11):E648-E659. doi:10.1097/BRS.0000000000001925
Adamson T, Godil SS, Mehrlich M, Mendenhall S, Asher AL, Mcgirt MJ. Anterior cervical discectomy and fusion in the outpatient ambulatory surgery setting compared with the inpatient hospital setting: analysis of 1000 consecutive cases. J Neurosurg Spine. 2016;24(6):878-84. doi:10.3171/2015.8.SPINE14284
Additional Reading
Mayfield Brain & Spine. Anterior Cervical Discectomy & Fusion.

By Brett Sears, PT
Brett Sears, PT, MDT, is a physical therapist with over 20 years of experience in orthopedic and hospital-based therapy.







Post comments