
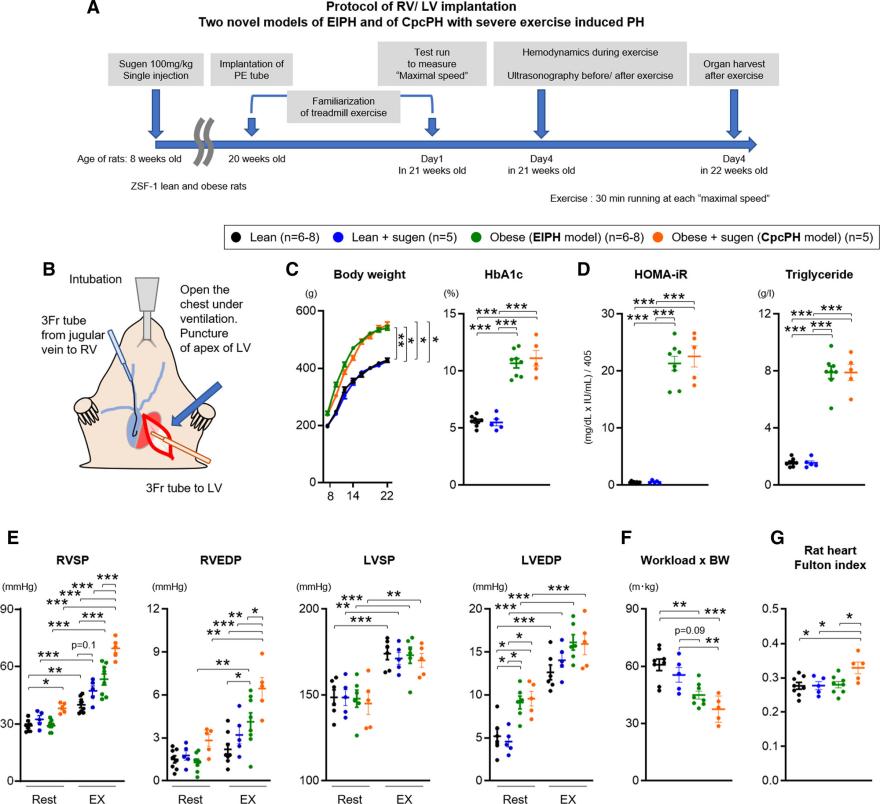
Novel HFpEF rat and CpcPH model of EIPH. A, Experimental timeline for lean, lean treated with sugen, obese (EIPH model), and obese rats treated with sugen (CpcPH model). B, Representative image of implantation of a polyethylene (PE) tube in the right (RV) and left (LV) ventricles. C and D, At 22 weeks of age, body weight (BW), hemoglobin A1c (HbA1c) level, homeostatic model assessment for insulin resistance (HOMA-IR), and triglycerides were measured (lean n=8, lean+sugen n=5, obese n=8, obese+sugen n=5). E, RV systolic and end-diastolic pressures (RVSP and RVEDP) and LV systolic and end-diastolic pressures (LVSP and LVEDP) were measured at rest and during exercise (EX; lean n=6–8, lean+sugen n=5, obese n=6–8, obese+sugen n=5). F, Workload was calculated with the distance of test run and body weight (lean n=8, lean+sugen n=5, obese n=8, obese+sugen n=5). G, Fulton index was measured as weight of RV/weight of LV+septum in lean (n=8), lean+sugen (n=5), obese (n=8), and obese+sugen (n=5) rats. Results are expressed as mean±SEM. Comparisons of parameters were performed with the 2-tailed Student t test, Welch t test, 1-way ANOVA, repeated-measures 2-way ANOVA, or mixed-effects model analysis followed by the Tukey honestly significant difference test for multiple comparisons. CpcPH indicates combined precapillary and postcapillary pulmonary hypertension; EIPH, exercise-induced pulmonary hypertension; HFpEF, heart failure with preserved ejection fraction; and PH, pulmonary hypertension. *P<0.05. **P<0.01. ***P<0.001.
Heart failure with preserved ejection fraction (HFpEF) is a common and complex cardiac disease, accounting for over 50% of heart failure cases worldwide. Many patients with HFpEF suffer from metabolic syndrome and may develop exercise-induced pulmonary hypertension (EIPH). This high pulmonary vascular resistance often indicates a poor prognosis and is known as combined pre-capillary and post-capillary pulmonary hypertension (CpcPH). However, current treatments for EIPH and CpcPH are limited and generally ineffective. Therefore, understanding the specific mechanisms by which metabolic syndrome contributes to HFpEF and EIPH is crucial for identifying new therapeutic targets for this complex disease. Taijyu and colleagues used a rat model to investigate how metabolic syndrome downregulates soluble guanylate cyclase (sGC) through a ROS-miR-193b-NFYA dependent mechanism, further studying how this mechanism leads to exercise-induced EIPH in HFpEF patients.
The researchers began by dividing the rats into four groups: control, HFpEF, obesity, and CpcPH. An HFpEF rat model was created by knocking out the ZSF-1 leptin receptor in obese rats. To induce resting pulmonary hypertension and establish the CpcPH model, the researchers administered SU5416 to the obese ZSF-1 leptin receptor knockout rats. Subsequently, the CpcPH group rats were treated with the SGLT2 inhibitor Empagliflozin. Hemodynamic parameters of the left and right ventricles were measured in all rats at rest and during exercise using catheter implantation. Pulmonary artery function and structural changes were assessed through magnetic resonance imaging (MRI). Additionally, adeno-associated virus 6 was used to deliver and overexpress the transcription enhancer factor NFYA for the sGCβ1 subunit. Finally, immunofluorescence and immunoblotting were employed to detect the expression levels of NFYA, sGCβ1, ROS, and miR-193b in pulmonary artery smooth muscle cells.
The results indicated that the pulmonary arteries in the obese and CpcPH groups produced elevated levels of reactive oxygen species (ROS) and exhibited reduced expression of sGCβ1. Cultured pulmonary artery smooth muscle cells (PAVSMCs) from obese rats and diabetic patients, as well as cells treated with palmitic acid, glucose, and insulin, showed increased mitochondrial ROS production. This increase in ROS led to miR-193b-dependent degradation of NFYA mRNA, which resulted in diminished sGCβ1-cGMP signaling. Overexpression of NFYA via adeno-associated virus 6 delivery elevated sGCβ1 levels and ameliorated exercise-induced pulmonary hypertension (EIPH) in the CpcPH group rats. Treatment of CpcPH group rats with the SGLT2 inhibitor Empagliflozin improved metabolic syndrome, reduced mitochondrial ROS and miR-193b levels, restored NFYA/sGC activity, and prevented EIPH.
In summary, the study demonstrated that metabolic syndrome enhances mitochondrial ROS production and miR-193b expression, leading to NFYA-dependent downregulation of sGCβ1 expression. Overexpression of NFYA via adeno-associated virus and inhibition of SGLT2 can restore NFYA-sGCβ1-cGMP signaling and improve EIPH. These findings provide new models for understanding the pathophysiology of HFpEF and CpcPH, revealing novel therapeutic targets. The study suggests new treatment approaches, such as NFYA overexpression or SGLT2 inhibitors, to address the upstream mechanisms of exercise-induced pulmonary hypertension in HFpEF.
This study, through innovative ideas, methods, and models, profoundly reveals the molecular mechanisms linking metabolic syndrome to HFpEF and EIPH. It proposes new strategies for improving these conditions through gene therapy and pharmacological treatment. Compared to traditional methods, these new models more comprehensively simulate the complexity of human diseases, and the new methods provide more targeted therapeutic options. However, the study has certain limitations that require further efforts. These include in-depth mechanistic understanding, clinical validation, expansion of sample size, and multi-center studies to ensure the reliability of the research results and the feasibility of clinical application. These efforts will aid in developing more effective and safer treatments, ultimately improving patient prognosis and quality of life.
Future research in this direction may foster new technologies and investment opportunities, such as the development of gene therapies, ROS-regulating drugs, and multifunctional SGLT2 inhibitors. With advancements in technology and deepening research, these innovations are expected to significantly improve patient prognosis and quality of life.
Reference:
Satoh, Taijyu, et al. "Metabolic Syndrome Mediates ROS-miR-193b-NFYA–Dependent Downregulation of Soluble Guanylate Cyclase and Contributes to Exercise-Induced Pulmonary Hypertension in Heart Failure With Preserved Ejection Fraction." Circulation 144.8 (2021): 615-637.






Post comments