
by Università di Trento
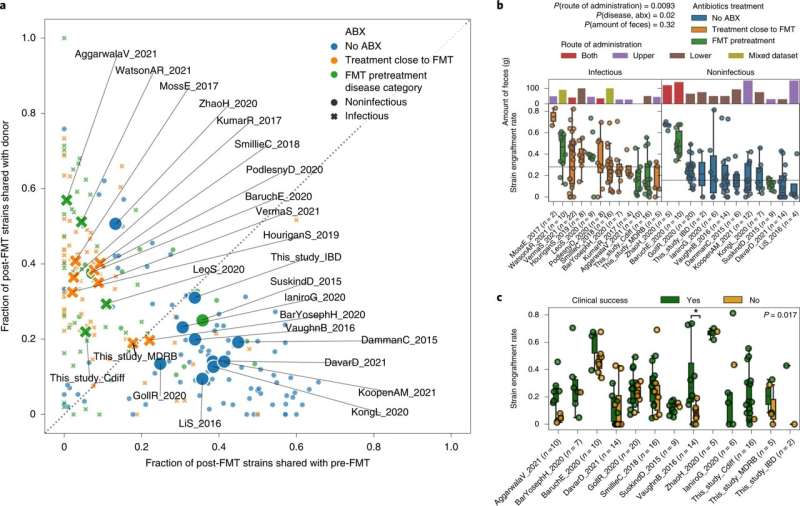
Variability of strain engraftment and retention across disease, antibiotics use and clinical success. a, Distribution of the fraction of donor strains and the fraction of retained strains present in the post-FMT samples for all FMT triads, showing a separation between higher fraction of donor strains and higher fraction of retained strains that associates with antibiotics administration and disease category. Small points represent individual FMT triads and large labeled marks represent per dataset averages. b, Variability of strain engraftment rate by disease category, antibiotics usage and route and amount of administered feces, highlighting the complex association between these variables and strain engraftment rates. The horizontal line is the median of per dataset medians. The statistical tests are performed by permuting the variables associated with datasets (two-tailed permutation test route of administration mixed versus lower or upper P = 0.0093, antibiotics and infectious disease versus no antibiotics and noninfectious disease in datasets employing single route of administration P = 0.02, amount of feces P = 0.32). c, Association between clinical success of FMT and strain engraftment rates for the 13 studies in which the information on clinical success was available and for which at least one recipient was in each group. The definition of clinical success for each study is reported in Supplementary Table 1. Permutation tests with success labels permuted within each dataset pointed at an overall significant association of strain engraftment with clinical success (two-tailed P = 0.017), that was significant in only 1 of the 13 datasets when considered individually (VaughnB_2016 Mann–Whitney U-test with two-tailed P = 0.039). Boxplots plots report the median and upper/lower quartiles, whiskers are at 1.5 times higher/lower of the upper/lower quartiles. Credit: Nature Medicine (2022). DOI: 10.1038/s41591-022-01964-3
From incurable intestinal infections to metabolic syndrome, from melanoma to chronic inflammatory bowel disease to Tourette's syndrome: Many diseases can potentially be cured by Fecal Microbiota Transplantation (FMT), and researchers from the Catholic University, Rome and the University of Trento have shown that the greater the level of engraftment of the transplanted microorganisms, the greater the chances of success of the therapy.
This is the core of the study published in the journal Nature Medicine.
"Microbiota transplantation," Antonio Gasbarrini, full professor of Internal Medicine at the Catholic University explains, "is a new therapeutic frontier that embraces different fields of medicine, not only gastroenterology, but even, for example, oncology."
Transplantation is done by isolating and purifying donor microbiota collected from feces and transferring it by various ways (in capsules or during a colonoscopy) to the donor patient. What is not really clear about this therapeutic procedure is how well the transplanted microorganisms engraft in the recipient patient's intestine.
Experts have analyzed with sophisticated genomic sequencing and computer analysis techniques a total of more than 1,300 gut microbiota samples (collected from feces) from donors and recipient patients with as many as eight different diseases (C. difficile, infections with intestinal multi-resistant bacteria, metabolic syndrome, melanoma, chronic inflammatory bowel disease, irritable bowel syndrome, chemotherapy diarrhea, Tourette's syndrome).
"Thanks to the ability of the analysis based on genomic sequencing techniques to identify the different bacterial strains present in the microbiota, which have a specific pattern for each person, we were able to understand whether a particular strain was transmitted from the donor to the recipient," Segata explains.
"We have seen that patients with higher levels of microbiota engraftment achieved a better clinical response; also that engraftment is greater in patients with infectious diseases (who have a less severe microbiota imbalance -dysbiosis) than in those with chronic diseases (who have more complex and radicate dysbiosis)," Ianiro says.
"We also found that patients treated with antibiotic therapy prior to the transplant procedure had higher engraftment, and that infusion of the microbiota via multiple routes of administration (e.g., capsules along with colonoscopy) promoted engraftment. It was also found that some microbial species (particularly Proteobacteria and Actinobacteria) engraft better than others (e.g., the phylum Firmicutes)."
"We have shown that by using artificial intelligence we can predict with relevant accuracy the composition of the donor microbiota after transplantation, and this could then lead to identifying the best donors whose feces are more successful in increasing the diversity of the microbiota (which is a parameter of microbiota health) post-fecal transplantation," say Ianiro and Segata.
"This study is the result of a fruitful collaboration and years of study by our research group on gut microbiota transplantation. It is thanks to these advances in knowledge about the conditions that maximize the success of transplantation that we will increasingly be able to exploit the procedure in clinical practice for the treatment of many diseases," says Giovanni Cammarota, Associate Professor in Gastroenterology at the Catholic University.
More information: Nicola Segata, Variability of strain engraftment and predictability of microbiome composition after fecal microbiota transplantation across different diseases, Nature Medicine (2022). DOI: 10.1038/s41591-022-01964-3. www.nature.com/articles/s41591-022-01964-3
Journal information: Nature Medicine
Provided by Università di Trento





Post comments