
by American College of Rheumatology
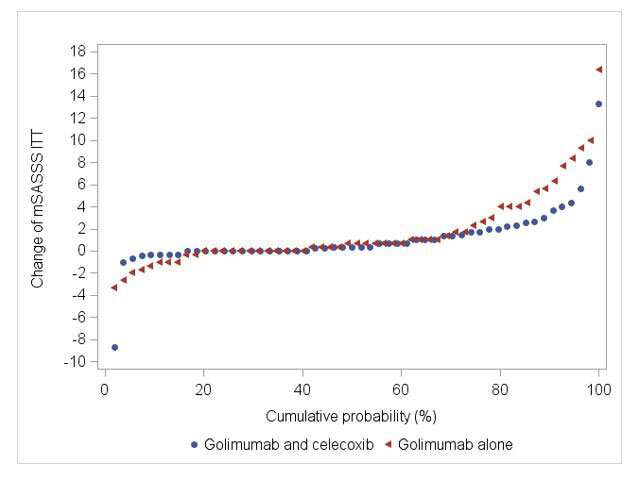
Cumulative probability plot of mSASSS progression over 108 weeks of treatment. Credit: COmparison of the Effect of Treatment with NSAIDs Added to Anti-TNF Therapy versus Anti-TNF Therapy Alone on Progression of StrUctural Damage in the Spine over Two Years in Patients with Ankylosing Spondylitis (CONSUL): An Open-Label, Randomized Controlled, Multicenter Trial (2022).
New research presented this week at ACR Convergence 2022, the American College of Rheumatology's annual meeting, showed that combining a nonsteroidal anti-inflammatory drug and TNF inhibitor did not significantly slow radiographic spinal progression in radiographic axial spondyloarthritis patients.
Axial spondyloarthritis (axSpA) is a chronic inflammatory condition with two subsets: non-radiographic axial spondyloarthritis and radiographic axial spondyloarthritis, the progressed stage of the disease. Radiographic axial spondyloarthritis was formerly known as ankylosing spondylitis.
Unlike non-radiographic, radiographic axSpA is marked by evidence of structural damage on X-rays. The main clinical symptom is back pain, with active inflammation in the sacroiliac joints and spine and in some patients, excessive new bone formation that can impair function.
"Reduction of clinical burden and prevention of disability can probably be best achieved by early and adequate treatment targeting both inflammation and new bone formation," says Fabian Proft, MD, a rheumatologist and senior researcher at Charité Universitätsmedizin Berlin and the study's lead author.
Continuous use of celecoxib, a selective nonsteroidal anti-inflammatory drug (NSAID), may be associated with less radiographic progression in radiographic axSpA patients. Biologic disease-modifying anti-rheumatic drugs (DMARDs) are often used to treat high disease activity, and the extent to which they impair structural damage remains ambiguous, Dr. Proft says.
"The effect on radiographic progression in radiographic axSpA of a combined treatment of biologic DMARD plus NSAID has not been investigated so far. We wanted to evaluate the impact of celecoxib when added to a biologic DMARD. This study used the tumor necrosis factor inhibitor (TNFi) golimumab with celecoxib and compared it to golimumab alone on progressive structural damage in the spine over two years in patients with active radiographic axSpA."
Eligible patients for this prospective randomized controlled trial were recruited from centers throughout Germany. All had a clinical diagnosis of radiographic axSpA, fulfilled the modified New York criteria for ankylosing spondylitis, had high disease activity despite NSAID therapy, and had at least one additional risk factor for radiographic progression (elevated C-reactive protein and/or already existing syndesmophytes [bony growths inside spinal ligaments]).
The trial had two phases. The first was a 12-week run-in phase in which participants received 50 mg of golimumab every four weeks. Those who had a good clinical response were equally randomized to the combination group (400 mg a day of celecoxib plus golimumab) or the golimumab only control group for 96 weeks.
Ninety-seven of the original 109 randomized patients completed the trial. Patients in the combination group had a change in the Stoke Ankylosing Spondylitis Spine Score of 1.1 points compared to a 1.7 change in the control group. Three blinded readers identified new syndesmophytes in 11% of the combination group versus 25% golimumab only group, respectively. During the study, seven serious adverse events were reported in the combination group compared to five in the control group. Two occurred during the run-in phase.
Overall, the observed differences between the combination treatment and monotherapy did not reach statistical significance.
"We did not expect that," Dr. Proft says.
"[It might be possible that] the findings would have become statistically significant with a larger sample size or longer follow-up, such as four years. [But] based on our data, continuous treatment with NSAIDs in addition to a biologic DMARD solely to inhibit future radiographic progression cannot be generally recommended. However, the observed effect of a combined treatment might be relevant in patients with a high risk for radiographic progression or with residual symptoms despite biologic DMARD therapy."
More information: Conference abstract
Conference: www.rheumatology.org/Annual-Meeting
Provided by American College of Rheumatology







Post comments