
by Ríona Mc Ardle, Public Library of Science
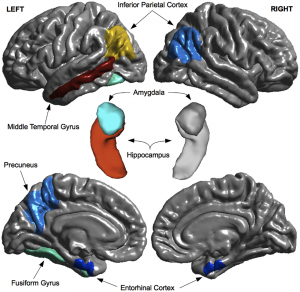
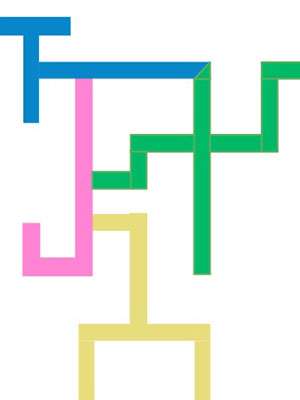
Regional MRI predictors of MCI-to-dementia progression. Figure courtesy Korolev et al. via PLOS One.
This eloquent quote by V.S. Ramachandran expresses the feelings of many of the people around the world who are celebrated Brain Awareness Week (#BAW2016), which occurs annually in March. This global campaign strives to inform the public about the marvels science has discovered about the brain and the benefits this research holds for all of us. Alongside enlightening discoveries about how the brain shapes our understanding of the world, researchers use various methods to improve diagnostics, and locate the causes and develop cures to brain diseases.
Alzheimer's disease (AD), a neurodegenerative disorder characterised by its notable memory impairment, has become a beacon for brain research. The need for more research is further evident, as patient numbers are set to increase from 44 million people living with AD today to 135.5 million people worldwide afflicted by 2050. The growing global burden of AD will lead to significant economic and social costs, and governments all over the world – such as the UK, USA and Australia – have pledged more funding for research in an effort to fight the disease. Identifying early diagnostic markers is pivotal in AD research. Indicators that can allow for early diagnosis of AD is important for two key reasons: (1) to allow individuals and their family valuable time to accept the diagnosis and adapt their lives accordingly and (2) to understand the factors contributing to disease progression. By identifying early diagnostic markers, researchers are exploring the neural systems affected in the early stages of AD, and informing treatments and interventions that could slow down or modify the course of the disease.
How do we investigate risk of Alzheimer's Disease?
Mild Cognitive Impairment (MCI) is viewed as a pre-dementia stage for AD and other dementias, and has improved our understanding of AD progression. MCI refers to a noticeable change in an individual's cognition in one or more domains, such as memory or the ability to pay attention, but functional abilities preserved – such as the ability to pay bills, shop or prepare a meal. These individuals are able to remain independent and are not diagnosed with dementia. MCI could provide an insight into the aetiology of AD and flag risk factors for the progression of dementia and transition to the disease. Researchers are exploring various avenues concerning early diagnostic markers – from investigating the neuropsychological changes to searching for structural brain changes across time.
A recent study in PLOS ONE tested a multivariate prognostic model to predict the transition from MCI to AD using baseline data of 289 MCI subjects collected for the Alzheimer's Disease Neuroimaging Initiative. These patients were placed in two groups, those who progressed to a diagnosis of probable AD within 36 months (p-MCI) and those who did not (n-MCI). The researchers chose to include data that would be routinely collected during a clinical assessment of dementia, such as brain scans from magnetic resonance imaging (MRI), cognitive and functional assessments, and blood samples. These resources provided more than 750 variables for the multivariate prognostic model. A thorough cross-validation framework was applied to assess predictive utility. The researchers used a method called Multiple Kernel Learning, which uses algorithms to integrate data from different sources and derive similarities between them based on their features. In short, this marked out which variables were best able predict progression from MCI to AD.
The results suggested that assessments of cognition and functionality were the best predictors for disease progression, with the Alzheimer's Disease Assessment Scale, Functional Activities Questionnaire and Rey Auditory Verbal Learning Task best predicting the transition from MCI to AD. The p-MCI group demonstrated more cognitive deficits in these assessments than the n-MCI group at baseline. The hippocampal, inferior parietal and middle temporal regions of the brain also showed reduced volume in the p-MCI group at baseline in comparison to the n-MCI group – this also acted as a predictor for progression to AD. These areas are involved in memory, interpretation of sensory input and language abilities. Blood-based plasma proteomic data was the least predictive marker, failing to accurately distinguish between the two groups. The variety of neuropsychological tasks and brain areas as predictors suggests that subtle impairments in cognitive domains, aside from memory, may be a risk factor for AD. This study provided evidence of the predictive properties of routine clinical tests for AD, a beneficial approach, as these resources are easily accessible and cost effective.
Why is identifying diagnostic markers for Alzheimer's Disease important?
While MCI can be an early indicator of Alzheimer's disease, it can also develop into other forms of dementia or in some cases, remain stable. Misdiagnosis between the dementia subtypes is common, particularly between dementia with Lewy bodies and AD – with rates of misdiagnosis as high as 83% reported. This can have a severe impact on patients' lives as accurate diagnosis is essential for appropriate treatments and interventions. Early diagnostic markers could strengthen the diagnosis of AD and improve management and treatment of the disease.
While the idea of finding early diagnostic markers for AD seems a relatively simple suggestion, it is complicated. The models developed to predict the progression from MCI to dementia can only be as accurate as the clinical diagnosis of the disease. Because the clinical and pathological presentation of AD is notably heterogeneous, currently the only definitive way to ascertain the diagnosis is through post-mortem investigation of changes in the patients' brain. The study described earlier fails to follow patients up to this stage and also ignores a range of other possible diagnostic markers, such as cerebrovascular fluid. While the study makes positive steps towards a more robust method for assessing risk factors for AD, more research is necessary, including replication studies and comparisons with other forms of dementia could benefit these findings.
One of the core things emphasized during Brain Awareness Week is the importance and necessity of brain research. Through research in dementia and the variety of markers that predict risk of the disease, scientists are conducting research to benefit our health and longevity.
More information: Albert, M. S., DeKosky, S. T., Dickson, D., Dubois, B., Feldman, H. H., Fox, N. C., … & Snyder, P. J. (2011). The diagnosis of mild cognitive impairment due to Alzheimer's disease: Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer's & dementia, 7(3), 270-279.
Kenigsberg, P. A., Aquino, J. P., Bérard, A., Gzil, F., Andrieu, S., Banerjee, S., … & Platel, H. (2015). Dementia beyond 2025: Knowledge and uncertainties. Dementia, 1471301215574785.
Korolev, I. O., Symonds, L. L., Bozoki, A. C., & Alzheimer's Disease Neuroimaging Initiative. (2016). Predicting Progression from Mild Cognitive Impairment to Alzheimer's Dementia Using Clinical, MRI, and Plasma Biomarkers via Probabilistic Pattern Classification. PloS One,11(2), e0138866.
Ramachandran, V. S. (2012). The tell-tale brain: A neuroscientist's quest for what makes us human. WW Norton & Company.
Riverol, M., & López, O. L. (2011). Biomarkers in Alzheimer's disease. Front Neurol, 2, 46.
Tiraboschi, P., Salmon, D. P., Hansen, L. A., Hofstetter, R. C., Thal, L. J., & Corey-Bloom, J. (2006). What best differentiates Lewy body from Alzheimer's disease in early-stage dementia?. Brain, 129(3), 729-735
Journal information: PLoS ONE , Brain
Provided by Public Library of Science
This story is republished courtesy of PLOS Blogs: blogs.plos.org.
Team suppresses oxidative stress and neuronal death associated with Alzheimer's disease
by Institute for Basic Science
The brain is an enormous network of communication, containing over 100 billion nerve cells, or neurons, with branches that connect at more than 100 trillion points. They are constantly sending signals through a vast neuron forest that forms memories, thoughts and feelings; these patterns of activity form the essence of each person. Alzheimer's disease (AD) disrupts both the way electrical charges travel within cells and the activity of neurotransmitters. An AD brain has fewer nerve cells and synapses than a healthy brain; plaques and abnormal clusters of protein fragments accumulate between nerve cells. The major pathological indicators of AD are the accumulation of amyloid beta plaques and neurofibrillary tangles in the brain. The pathways in our neuron forest are systemically attacked and destroyed by amyloid beta (Aβ): a solitary molecule that evolves into plaque clusters, which block cell-to-cell signalling at synapses. They may also activate immune system cells that result in inflammation and destroy damaged cells.
Deterioration of the Brain
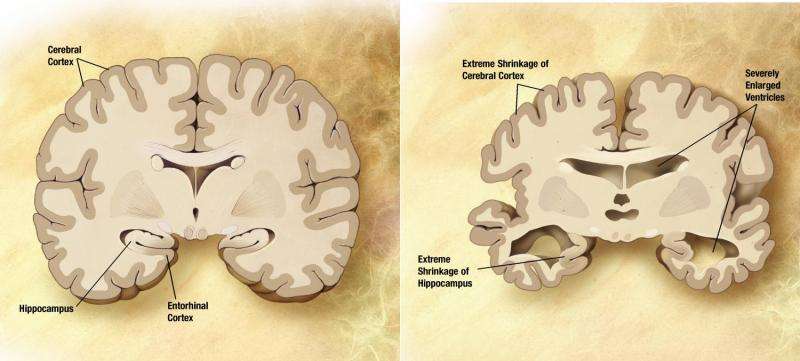
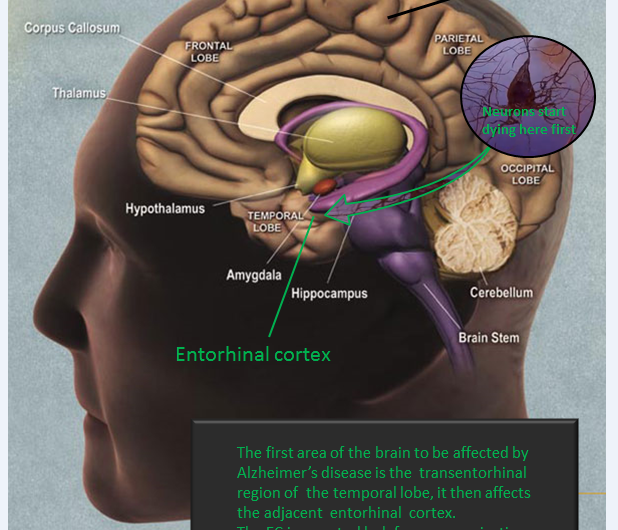
In a healthy brain, orderly parallel strands, akin to railroad tracks, permit nutrients and essential proteins to move between cells. The protein tau helps these tracks remain intact and functioning. In an AD affected brain tau breaks down, collapses and forms tangles that prevent transmission along the tracks. The tracks fall apart and disintegrate. Essential proteins, including nutrients, can no longer reach brain cells, which eventually die. The plaques and tangles described above are currently the leading working theory explaining the cell death and tissue loss found in an AD brain, though the theory is yet to be irrefutably confirmed. The effects of AD on the brain, however, are well known: brain cells slowly disintegrate, the disease progressively invades different parts of the brain, creating unique changes that signal the various stages of Alzheimer's. Short term memory loss, logical thoughts and emotions are all obstructed, fundamentally altering and ultimately eradicating an affected individual's personality. Over time, Alzheimer's leads to nerve cell death and dramatic shrinking of the brain, which affects nearly all of its functions.
Stemming Tangles and Plaques
The scientific team from the Center for Nanoparticle Research within the Institute for Basic Science (IBS) has developed a novel mitochondria-targeting ceria nanoparticle that can effectively impede the process of neuronal cell death, in collaboration with the research group of Seoul National University led by professor Inhee Mook. Cells in our brain are powered by mitochondria; tiny power plants within cells that produce a body's essential energy, which is required for each cell to function. Reactive oxygen species (ROS) are formed as a natural by-product of normal metabolism of oxygen. Abnormal generations of ROS, resulting from mitochondrial dysfunction, can lead to neuronal cell death. Additionally, Aβ-induced mitochondrial dysfunction also has been known to be a possible cause of AD through abnormal production of ROS. Ceria nanoparticles function as known to function as strong and recyclable ROS scavengers, eliminating abnormal ROS, by shuttling between Ce3+ and Ce4+ oxidation states.
Suppressing Neuronal Death
The research team, under the direction of the IBS Center's director Taeghwan Hyeon, synthesized a ceria nanoparticle, mitochondria-specific antioxidant and investigated the effect of the new therapeutic agent in suppressing the pathogenesis of AD using an in vivo mouse model. The team introduced the powerful ceria nanoparticles (CeO2 NP) to mitochondria by using small, mitochondria-targeting materials (triphenylphosphonium-conjugating) and recorded quite remarkable results in a transgenic AD mouse model. Two months after the mouse was injected, positive cells were quantified. According to the results, published online in ACS Nano on February 11, the CeO2 NPs localised to mitochondria had effectively suppressed neuronal death in the mouse model, demonstrating that the administration of mitochondria-targeting ceria NPs significantly restored neuronal viability of the AD-affected mouse. Since the accumulation of Aβ did not differ significantly between the brains of the affected and non-treated mouse, it is concluded that the mitochondria-targeting ceria NPs ameliorate the neuronal damage of the test subject in an indirect way, independent of the Aβ accumulation. The team's paper stressed that the data "indicated that the mitochondria-targeting ceria NPs are a potential therapeutic candidate for treating mitochondrial oxidative-stress-induced damage in AD." Director Hyeon said, "This study is quite remarkable in that the collaborative research between nano science and biomedical science has led to a potent therapeutic agent against reactive oxygen species in the mitochondria, which is deemed to be one of major culprits in a number of diseases.
More information: Hyek Jin Kwon et al. Mitochondria-Targeting Ceria Nanoparticles as Antioxidants for Alzheimer's Disease, ACS Nano (2016). DOI: 10.1021/acsnano.5b08045
Journal information: ACS Nano
Provided by Institute for Basic Science





Post comments