
by Stanford University Medical Center
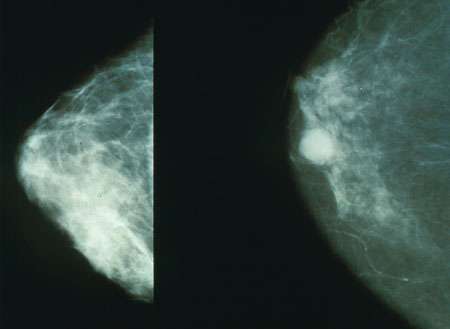
Mammograms showing a normal breast (left) and a breast with cancer (right). Credit: Public Domain
In the last few decades, dozens of new breast cancer drugs—from chemotherapies to targeted compounds—have become available for clinical use, and mammogram technology has gone from film to digital. But are the changes making a difference in how many women die of breast cancer?
The answer to that question is a resounding yes, according to a multi-institutional network of researchers who have modeled the effect of breast cancer screening and treatment on mortality rates.
The researchers' models showed that screening and treatment reduced breast cancer mortality by 49 percent in 2012, compared with 37 percent in 2000.
"These numbers represent very positive news for breast cancer patients," said Sylvia Plevritis, PhD, professor of radiology and of biomedical data science at the Stanford University School of Medicine and lead author of the paper, which will be published Jan. 9 in JAMA. "Advances in screening and treatment are saving patients' lives, and this paper quantifies just how much of a difference these advances are making."
An international effort
In 2005, Plevritis and her colleagues in the Cancer Intervention and Surveillance Modeling Network used data from 1975 through 2000 to reveal the relative contributions of screening and treatment to reductions in breast cancer mortality rates. Using knowledge of how breast cancer advances, they developed models representing how many women would die of the cancer with no screening and no treatments, then simulated the effect of screening and treatment on those mortality numbers.
The decrease in mortality from the modeled baseline, they found, was about 50 percent due to screening and 50 percent due to treatment.
"Now, over 10 years later, a lot has happened in the field," said Plevritis, who heads the Stanford Center for Cancer Systems Biology. "We've moved from film-based mammography to digital; there are new molecularly targeted treatments and new types of chemotherapy regimens. We wondered whether these advances had changed the relative contributions of treatment and screening on breast cancer mortality."
So researchers in the network updated their models to reflect molecular subtypes of breast cancer. Six independent teams—including researchers from Stanford, the Dana-Farber Cancer Institute, Erasmus Medical Center, Georgetown University Medical Center, Albert Einstein College of Medicine, the University of Wisconsin, Harvard Medical School and MD Anderson Comprehensive Cancer Center—put together models representing the effect of current treatment and screening.
The group added new data—spanning 2000 to 2012—to the existing data and compared the conclusions of each model, calculating average effects on mortality of screening and of treatments, including chemotherapy, hormone therapy and the drug trastuzumab, which targets an epidermal growth factor receptor, ERBB2, overexpressed in some tumors. By comparing six models, the researchers were able to replicate the analysis, making the team more confident in results that were seen in all the models. Not only did they look at the effects on breast cancer as a whole, but on molecular subtypes of breast cancer, such as those that are ER positive, meaning that they grow in response to the hormone estrogen.
"This time around, it was important to look at molecular subtypes because more women are being treated based on the molecular subtype of their tumor," Plevritis said.
Subtype matters
The researchers found that in 2012, screening and treatment together reduced breast cancer mortality by 49 percent. For all breast cancers together, 37 percent of that reduction was due to screening, and 63 percent was due to treatment.
However, when they looked at some molecular subtypes of cancer, the numbers varied. For ER-positive/ERBB2-positive cancer, the most common type and the type for which the greatest number of new targeted treatments are available, only 31 percent of the mortality decline was associated with screening, with 69 percent associated with treatment. For ER-negative/ERBB2-negative cancer, which has fewer treatment options, 48 percent of the mortality decline was associated with screening and 52 percent with treatment, similar to results from 2000.
"Newer drugs, particularly ones that are molecularly targeted, are associated with a greater reduction in breast cancer mortality than screening," said Jeanne Mandelblatt, MD, MPH, professor of oncology and of medicine at Georgetown University and a senior author of the paper. "However, screening is still having a significant effect in reducing breast cancer deaths."
In particular, the researchers pointed out, screening can lead to cancer detected at earlier stages and therefore less-intense treatments. Aside from reducing mortality rates, this can translate into fewer side effects and patient co-morbidities.
Plevritis said the new results are useful for researchers and policymakers who must make decisions on how to prioritize new efforts to advance breast cancer treatment and screening.
"There have been many investments in screening and treatment; we want to know what impact those investments have had in reducing mortality," she said. "It also helps us think about the future and how to make sure technologies and drugs that are making the biggest difference are disseminated most widely."
The work is an example of Stanford Medicine's focus on precision health, the goal of which is to anticipate and prevent disease, as well as to precisely diagnose and treat disease.
Journal information: Journal of the American Medical Association
Provided by Stanford University Medical Center







Post comments