
by Cleveland Clinic
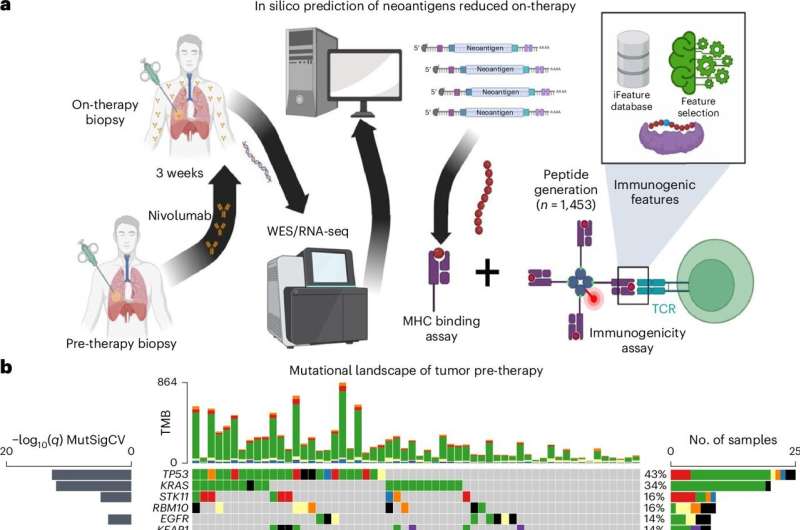
Neoantigen screening design and genomic features of NSCLC cohort. a, WES was performed on n = 58 pre-therapy samples and n = 42 on-therapy samples, which includes n = 36 cases with matched pre-/on-therapy data. After neoantigen prediction n = 14 patients underwent immunogenicity screening, and the subsequent data were used to model features driving immunogenicity. b, Mutational landscape pre-therapy of common somatic mutations in NSCLC (n = 58). Top 3 mutational signature scores by DeconstructSig (SBS1, SBS4, SBS87). Frequency of clonal/sub-clonal variants (defined by ≥0.95 blue bar CCF or <0.95 CCF red bar). Fraction copy number change per samples represented as bar plot (bottom panel). del, deletion; ins, insertion; NSQ, nonsquamous; SQ, squamous. Credit: Nature Medicine (2024). DOI: 10.1038/s41591-024-03240-y
A Cleveland Clinic-led research collaboration between Timothy Chan, MD, Ph.D., Chair of Cleveland Clinic's Global Center for Immunotherapy, and Bristol Myers Squibb has published the most comprehensive overview to date of how the immune system reshapes tumor architecture in response to immune checkpoint therapy.
The eight-year study, published in Nature Medicine, outlines how cancer immunotherapy induces tumor recognition through neoantigens to reshape the tumor ecosystem. Neoantigens are small peptides produced when cancer cells mutate and are a primary marker for the immune system to recognize cancer cells as different from self.
"This study is unique in that we sampled tumors prior to therapy and then early after immunotherapy was initiated," explains Dr. Chan, who is also chair of Cleveland Clinic's Center for Immunotherapy & Precision Immuno-Oncology, program leader of Case Comprehensive Cancer Center's Immune Oncology Program and the Sheikha Fatima bint Mubarak Endowed Chair in Immunotherapy. "Our goal was to understand how patients' tumors are recognized and altered by their immune system in response to immunotherapy."
Our immune cells and cancer cells constantly interact and influence one another over the course of cancer. Immunotherapy treatments need to operate within that framework by boosting our immune cells to eliminate cancer. Scientists like Dr. Chan have begun to untangle the complex relationships among treatment, immunity and cancer in the past 15 years—but human data is in short supply.
The CheckMate-153 trial was overseen by pharmaceutical company Bristol Myers Squibb and Dr. Chan's team was a central site for the trial's analysis. Within the primary trial, investigators included a biomarker sub-study to identify how neoantigens drive response to nivolumab by sampling patients' tumors pre-therapy and 3 weeks post-therapy. From these tumor samples, sequencing was used to identify mutations that create neoantigens.
Neoantigens are thought to be the primary way that the immune system recognizes tumors, but neoantigen prediction tools lack accuracy due to a lack of existing data in this space. To overcome this issue, the team developed the largest neoantigen screen to date, where they validated their predictions and monitored the dynamic response to neoantigens with longitudinal blood draws.
Within three weeks of treatment, people who went on to respond well to nivolumab had a sharp decline in clonal neoantigens. Meanwhile, individuals whose cancer did not go into remission still mounted an immunologic response, but to smaller sub-clonal populations. This is important because many believed that non-responders were unable to activate and recognize the tumor, but here they show it may be that the immune system is mounting a response to neoantigens but that this is insufficient to destroy all tumor clones.
Current neoantigen prediction tools rely heavily on HLA-binding neoantigens, but they are missing the T cell recognition aspect of immunogenicity, says Cleveland Clinic's co-first author Tyler Alban, Ph.D., Project Staff in the Chan Lab. Dr. Alban, data scientist Prerana Parthasarathy, and others on the team developed a machine-learning program that uses the new screening data to better predict immunogenic neoantigens. In the process, the program identified novel features harbored by these cancer-derived neoantigens.
"We observed a whole ecosystem of immune cells at work, with each T cell recognizing a different neoantigen altering the clonal makeup of the tumor," Dr. Alban says. "Our data let us generate new insights into neoantigens and resistance to immunotherapy."
By cataloging changes to neoantigens during treatment, Dr. Alban's analyses challenged the prevailing theory in immunotherapy: that a tumor only needs one lucky mutation to develop features our immune systems recognize as a threat. The results show that many different T cells recognizing many different cancer-causing features are needed to respond well to treatment.
Roadmaps generated by these types of observational studies will be critical in navigating future immuno-oncology research, Dr. Chan says.
"Learning why our immune systems respond to some cancerous mutations but not others is like the holy grail for immunotherapy researchers," he explains. "Our findings are one of the closest things we have to figuring these things out."
The group is also using their dataset in collaboration with IBM in the Cleveland Clinic—IBM Discovery Accelerator to develop more advanced AI models that predict new molecules for cancer treatments and cancer vaccine development.
More information: Tyler J. Alban et al, Neoantigen immunogenicity landscapes and evolution of tumor ecosystems during immunotherapy with nivolumab, Nature Medicine (2024). DOI: 10.1038/s41591-024-03240-y
Journal information: Nature Medicine
Provided by Cleveland Clinic







Post comments