
by Brunel University of London

Credit: Pixabay/CC0 Public Domain
A major U.K. study of more than 165,000 dementia patients has found that risperidone raises stroke risk without exception, challenging safety assumptions by leaving no "safe group."
The powerful anti-psychotic is commonly used to treat dementia patients experiencing severe agitation, especially incare homeswhere other strategies have failed.
Butstroke riskamongdementia patientstakingrisperidonerose even in people with no history of heart disease or stroke. This counters assumptions about safety and raises questions about how the drug, the only licensed drug of this type for use in dementia, is used and monitored.
The findings,publishedin theBritish Journal of Psychiatry, will likely prompt calls for changes in clinical practice.
Most striking was how consistent the risk was across all groups. "We knew risperidone causes stroke, but we didn't know whether some groups of people might be more at risk than others. We thought if we might identify characteristics that make people more at risk, doctors could avoid prescribing to patients with those characteristics," said Dr. Byron Creese from the College of Health, Medicine and Life Sciences at Brunel University of London.
Of people with dementia, 50% experience agitation, often causing severe distress. When non-drug treatments don't work, doctors may turn to risperidone as a last resort. The findings sharpen the already difficult choices facing doctors and families, who must weigh the serious stroke risks of risperidone against its potential to relieve extreme distress.
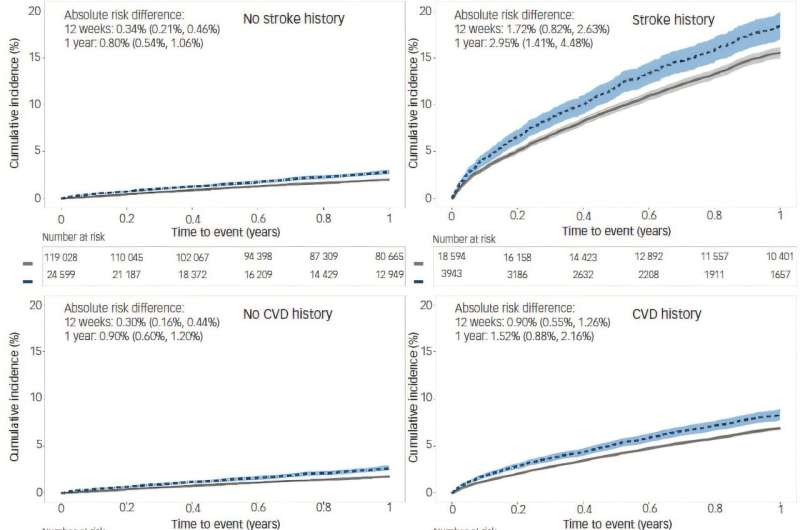
Kaplan–Meier plots depicting the cumulative incidence of stroke in matched controls and risperidone users. Blue dashed line indicates risperidone users. Credit:The British Journal of Psychiatry(2025). DOI: 10.1192/bjp.2025.10419
The drug, used to calm aggression, carries known risks of stroke inolder patients. Yet there is still no dementia-specific guidance on how doctors should monitor those dangers. NHS guidelines limit risperidone use to six weeks forsevere symptoms, but many patients take it for longer, with monitoring standards varying across the country.
There are no U.K. licensed alternatives for risperidone in such cases, says Dr. Creese, so it is about making sure the risks are clearly explained and carefully weighed up. People with a history of stroke already face a high risk of another stroke. If a stroke happens after taking risperidone, it may not be just because of the drug. Doctors only use risperidone as a last resort.
"These findings give clearer information about who is most at risk, which helps everyone make more informed choices. Every decision should be based on what is right for each person, through honest conversations between doctors, patients, and families."
The team analyzed anonymized NHS records between 2004 and 2023, comparing patients prescribed risperidone with matched controls who were not. In people with a history of stroke, the annual rate per 1,000 people jumped to 22.2% on risperidone, compared with 17.7% in those not taking it. In patients who'd not had astroke, the rates were lower but still significant—2.9% versus 2.2%. And the risk was higher in patients taking the drug over the short term (12 weeks).
"We hope that these data can be used in updated guidance that is more person centered and based on particular patient characteristics," said Dr. Creese.
More information: Joshua Choma et al, Risk of stroke associated with risperidone in dementia with and without comorbid cardiovascular disease: population-based matched cohort study, The British Journal of Psychiatry (2025). DOI: 10.1192/bjp.2025.10419 Journal information: British Journal of Psychiatry
Provided by
Brunel University of London






Post comments