
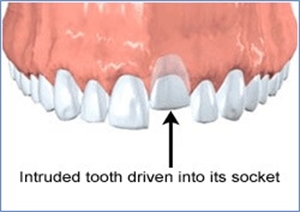
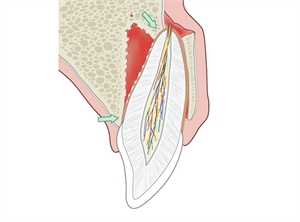
Tooth intrusion is one of the most severe forms dental injuries. The tooth is placed within the bone in a socket that supports it and also helps in stress distribution. However, when the intensity of the traumatic injury in a vertical direction to the long axis of the tooth is extremely high, it results in the tooth getting further intruded into the socket, such that it fractures the underlying socket.
Tooth intrusion - clinical findings
The intruded tooth is immobile and since the displacement of the tooth is within the socket, it results in the tooth being position lower in relation to the normal bite. The condition is painful for the patient. While checking for the health of the periodontal tissues, the dental surgeon might perceive a metallic sound upon percussion.
In case of primary or deciduous teeth, things become even more complicated as the intruded tooth can impinge the underlying permanent successor. The tooth is barely visible through the oral cavity but can be palpated through the gingival tissues.
Radiographic findings we can notice in intruded teeth
Multiple radiographs are necessary in order to understand the depth till which the tooth has penetrate the socket and if at all there are more injuries to the surrounding structures. It also helps in measuring the level of intrusion compared to the normal position of the tooth. In case of primary teeth, a radiograph is mandatory to understand whether the tooth bud or germ of the permanent successor is affected or not. In many cases, the intruded tooth can cause deflection in the eruption path of the permanent successor.
Treatment for teeth with incomplete development of roots
When the intruded permanent tooth is still young, its roots yet to develop, at that time the treatment plan differs from the conventional methods. In this case, the tooth is monitored for a month to see if root development is taking place. If the root is developing, then it means the tooth will have the ability to extrude itself to its original position. However, if there is no development of the roots and the tooth becomes infected and resorption of the roots begins, then treatments to reposition the tooth should begin. This is done by orthodontic treatment (braces). Once the tooth is repositioned, root canal treatments are performed.
Treatment for teeth with completed root development
In cases where the intruded tooth is completely mature, the pulp of the tooth is usually rendered necrotic. In such cases, the root canal treatments are initiated after 2 weeks or as soon as the tooth gets into a favorable position. Root canal treatments in such cases might be prolonged than conventional root canal treatments as it can involve placement of antibiotic medications within the tooth to reduce the inflammation.
If the tooth is intruded for less than 3 mm, then the tooth should be monitored for 2 months to see if it can reposition itself. If it does not, then surgical reposition is done and the tooth is splinted in its new position for one month. If the level of intrusion is between 3 to 7 mm, then repositioning should begin immediately either surgically or orthodontically. Intrusion beyond 7 mm warrants for surgical repositioning.
In primary teeth, tooth should be allowed to reposition itself irrespective of the level of displacement. In some cases it can take up to as long as 1 year for the tooth to reposition itself. However, if the pediatric dentist feels that the intrusion has affected the permanent tooth bud then careful extraction of the primary tooth is done in a manner that the permanent tooth germ is not hampered.
Follow-up
It is recommended for cases with intrusion of teeth are followed-up for at least 5 years. While the initial recalls are frequent after 2 weeks, 4 weeks, 8 weeks and 12 weeks, the recall visits to follow should be at every 6 months. Radiographic monitoring is a mandate and the health of the tissues supporting the tooth structure is monitored.
Prognosis
A favorable prognosis is when the tooth remains asymptomatic with no resorption of teeth. In case of immature permanent teeth, continual root development is a highly promising prognosis. In primary teeth, re-eruption and no harm to permanent successor is favored.
The most commonly encountered unfavorable outcome of intruded tooth is its ankylosis. This means that the external surface of the roots of the tooth has completely fused to the socket and there is no chance of repositioning the tooth except surgical means. An abscess corresponding to the intruded tooth, resorption of the tooth and severe harm to the permanent successor are the unfavorable outcomes.
Tooth intrusion is a relatively severe condition in terms of dental trauma and must be addressed as a matter of emergency. Parents of pediatric patients must be explained about the possible long-term complications. Adolescents and adults on the other hand must be regular in their follow-up visits while simultaneously ensuring that there are no further traumatic blows in the orofacial region.






Post comments