
By Angelica Bottaro
Updated on September 22, 2023
Medically reviewed by Matthew Wosnitzer, MD
Prostate cancer affected close to 200,000 people in 2020. Fortunately, the prognosis of prostate cancer is usually positive because it typically grows and spreads slowly.
Only a small portion of cases turn out to be fatal. In fact, the 5-year-relative survival rate of prostate cancer is 97.8%.1
Prostate cancer is staged like most other solid tumor cancers. But, additional risk assessment tools are also used to help direct treatment, including whether surgery is needed.
This article explains what tools are used to stage cancer and assess risk, and how they are used to help make treatment decisions.

FatCamera / Getty Images
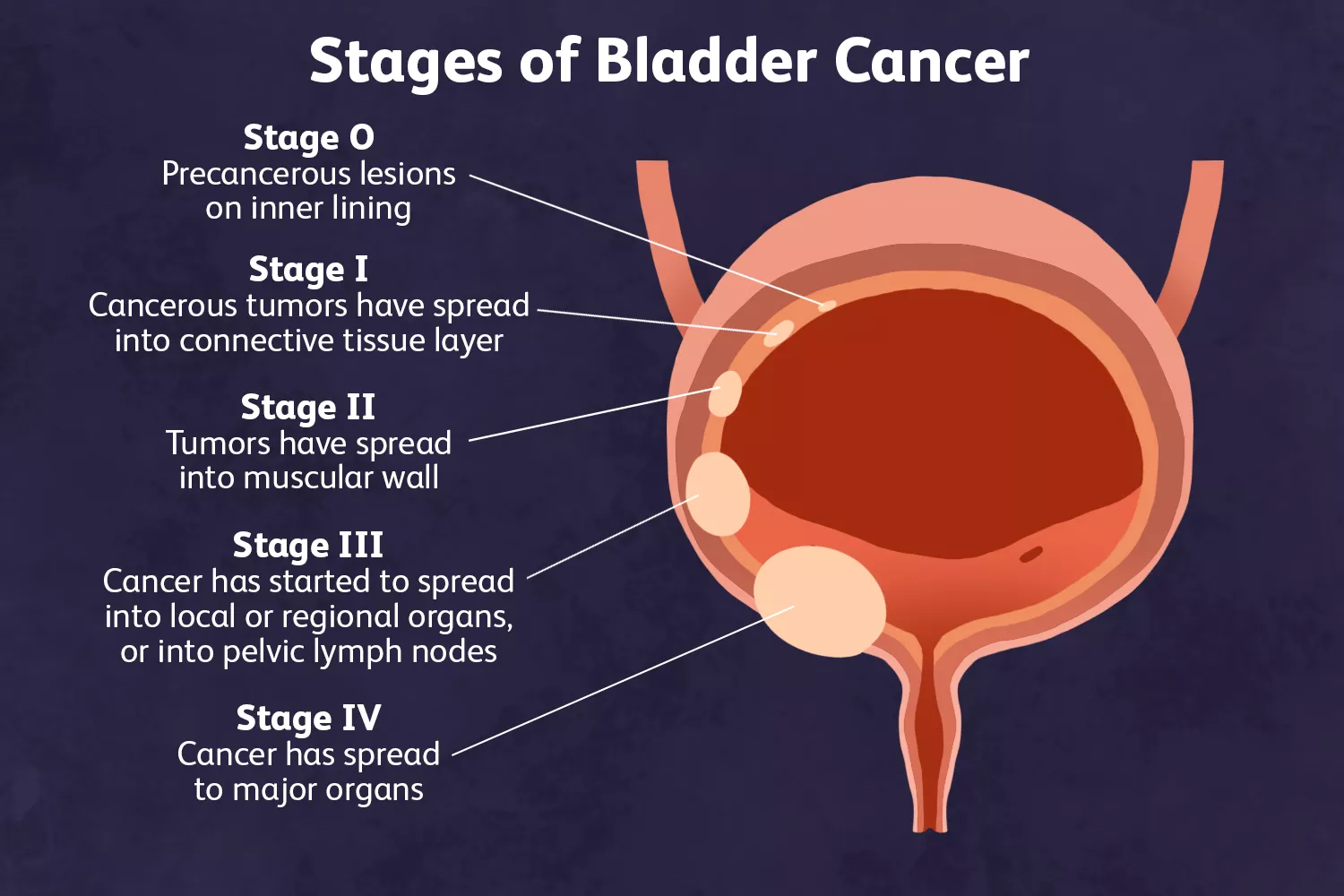
Prostate Cancer Staging
Healthcare providers stage cancer to determine how much cancer is within the body and if it has spread.2 This can help a person with cancer determine the best course of treatment and understand their chances of survival.
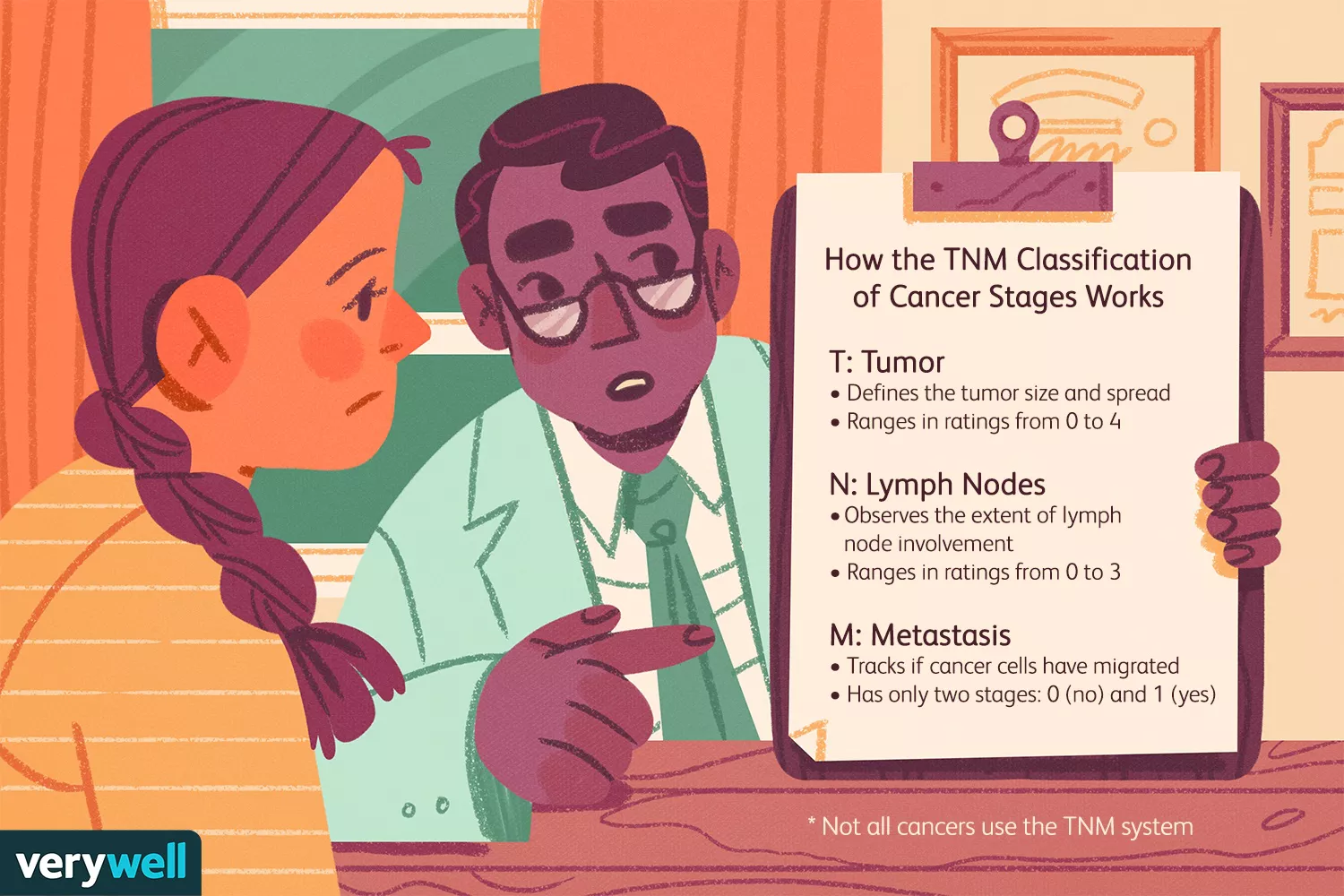
The TNM system developed by the American Joint Committee on Cancer (AJCC) is the most widely used cancer staging system. The acronym describes different factors about cancer, including:2
T (tumor): The size and extent of the main tumor
N (number): The number of nearby lymph nodes that have cancer
M (metastasis): Whether or not the tumor has spread to other parts of the body
Several tests and procedures are used to stage prostate cancer after a diagnosis is confirmed.
PSA Blood Test
A PSA blood test looks for increased levels of prostate-specific antigens (PSA) in the blood. When the test is used in those who have already been diagnosed with prostate cancer, it can help determine the stage of their cancer.
By combining elevated PSA levels with a physical exam and biopsy results, a healthcare provider can determine how much prostate cancer is in the body and whether or not it has spread to other parts of the body.3
Biopsy
Healthcare providers perform a biopsy for prostate cancer by removing a part of the prostate to check for abnormal cells and activity. The most common type of biopsy used is the core needle biopsy.
In this procedure, the healthcare provider inserts a long, thin, and hollow needle through the rectum or the skin between the anus and the scrotum to gather up to 12 samples. This is performed using ultrasound and/or MRI guidance.
A tumor grade is then assigned based on the results. The grade is determined by how abnormal the tumor looks under a microscope.3
American Cancer Society. Tests to diagnose and stage prostate cancer.
Gleason Score
The Gleason system assigns tumor grades based on how much the cancer looks like normal prostate tissue. The grades run from 1 to 5 (most normal to least normal). Almost all cases of prostate cancer are grade 3 or higher.3
Since prostate cancers often have areas with different grades, a grade is assigned to the two areas that make up most of the cancer. Then, these two grades are added to yield the Gleason score, which can be between 2 and 10.
Based on the score, prostate cancer is classified into three groups:
Well-differentiated or low-grade (a score of 6 or less)
Moderately differentiated or intermediate grade (a score of 7)
Poorly differentiated or high-grade (a score of 8 to 10)
However, the Gleason score may not always be the best way to describe the grade of cancer. That's because prostate cancer outcomes can be divided into more than just three groups, and the scale of the Gleason score can be misleading.3
Experts developed grade groups to help bridge the gaps. They range from 1 (most likely to grow and spread slowly) to 5 (most likely to grow and spread quickly). Grade Groups correspond to different Gleason scores:3
Grade Group 1: Gleason score of 6 or less
Grade Group 2: Gleason score of 3+4=7
Grade Group 3: Gleason score of 4+3=7
Grade Group 4: Gleason score of 8
Grade Group 5: Gleason score of 9 and 10
Stages of Prostate Cancer | ||
|---|---|---|
AJCC Stage | Stage Grouping | Stage Description |
I | cT1, N0, M0 Grade Group 1 PSA less than 10 OR cT2a, N0, M0 Grade Group 1 Gleason score 6 or less PSA less than 10 OR pT2, N0, M0 Grade Group 1 Gleason score 6 or less PSA less than 10 | The healthcare provider can’t feel the tumor or see it with an imaging test such as transrectal ultrasound (it was either found during a transurethral resection of the prostate or was diagnosed by needle biopsy done for a high PSA). The cancer has not spread to nearby lymph nodes or elsewhere in the body. OR The tumor can be felt by digital rectal exam or seen with imaging such as transrectal ultrasound and is in one half or less of only one side (left or right) of the prostate. The cancer has not spread to nearby lymph nodes or elsewhere in the body. OR The prostate has been removed with surgery, and the tumor was still only in the prostate. The cancer has not spread to nearby lymph nodes or elsewhere in the body. |
IIA | cT1, N0, M0 Grade Group 1 PSA at least 10 but less than 20 OR cT2a or pT2, N0, M0 Grade Group 1 PSA at least 10 but less than 20 OR cT2b or cT2c, N0, M0 Grade Group 1 PSA at least 10 but less than 20 | The healthcare provider can’t feel the tumor or see it with imaging such as transrectal ultrasound (it was either found during a transurethral resection of the prostate or was diagnosed by needle biopsy done for a high PSA level). The cancer has not spread to nearby lymph nodes [N0] or elsewhere in the body [M0]. OR The tumor can be felt by digital rectal exam or seen with imaging such as transrectal ultrasound and is in one half or less of only one side (left or right) of the prostate. Or the prostate has been removed with surgery, and the tumor was still only in the prostate. The cancer has not spread to nearby lymph nodes or elsewhere in the body. OR The tumor can be felt by digital rectal exam or seen with imaging such as transrectal ultrasound. It is in more than half of one side of the prostate or it is in both sides of the prostate. The cancer has not spread to nearby lymph nodes or elsewhere in the body. |
IIB | T1 or T2, N0, M0 Grade Group 2 PSA less than 20 | The cancer has not yet spread outside the prostate. It might (or might not) be felt by digital rectal exam or seen with imaging such as transrectal ultrasound. The cancer has not spread to nearby lymph nodes or elsewhere in the body. |
IIC | T1 or T2, N0, M0 Grade Group 3 or 4 PSA less than 20 | The cancer has not yet spread outside the prostate. It might (or might not) be felt by digital rectal exam or seen with imaging such as transrectal ultrasound. The cancer has not spread to nearby lymph nodes or elsewhere in the body. |
IIIA | T1 or T2, N0, M0 Grade Group 1 to 4 PSA at least 20 | The cancer has not yet spread outside the prostate. It might (or might not) be felt by digital rectal exam or seen with imaging such as transrectal ultrasound. The cancer has not spread to nearby lymph nodes or elsewhere in the body. |
IIIB | T3 or T4, N0, M0 Grade Group 1 to 4 Any PSA | The cancer has grown outside the prostate and might have spread to the seminal vesicles or other tissues next to the prostate, such as the urethral sphincter, rectum, bladder, and wall of the pelvis. It has not spread to nearby lymph nodes or elsewhere in the body. |
IIIC | Any T, N0, M0 Grade Group 5 Any PSA | The cancer might or might not be growing outside the prostate and into nearby tissues. It has not spread to nearby lymph nodes or elsewhere in the body. |
IVA | Any T, N1, M0 Any Grade Group Any PSA | The tumor might or might not be growing into tissues near the prostate. The cancer has spread to nearby lymph nodes, but has not spread elsewhere in the body. The Grade Group can be any value, and the PSA can be any value. |
IVB | Any T, any N, M1 Any Grade Group Any PSA | The cancer might or might not be growing into tissues near the prostate and might or might not have spread to nearby lymph nodes. It has spread to other parts of the body, such as distant lymph nodes, bones, or other organs. |
Recap
Healthcare providers categorize prostate cancer into stages. Staging helps determine how much cancer is in the prostate and if it has spread. Doctors rely on a PSA blood test, a biopsy, and Gleason score to determine the stage of prostate cancer.
Risk Groups
In people newly diagnosed with prostate cancer, healthcare providers will assess each case individually to determine how aggressive the tumor will likely be and the appropriate course of treatment.
The National Comprehensive Cancer Network (NCCN) developed guidelines to categorize prostate cancer into risk groups. They take into account blood test and exam results, genetic testing results, and family history to help determine the appropriate risk group:4
Very low: Includes people in the T1c stage, Grade Group 1, and who have a PSA of less than 10 ng/mL with PSA density being lower than 0.15 ng/mL, and if the cancer is found in one or two of the biopsies with less than half of all samples showing signs of cancer
Low: Includes people in the T1 to T2a stages, Grade Group 1, and a PSA of less than 10 ng/mL
Intermediate favorable: Includes people with one intermediate-risk factor who are in Grade Group 1 or 2 and have less than half of their biopsies showing cancerous results
Intermediate unfavorable: Includes people in Grade Group 3 with more than half of their biopsies showing cancer and having two or more intermediate risk factors
High: Includes people in the T3a stage or Grade Group 4 or 5 or those who have a PSA of more than 20 ng/mL
Very high: Includes people in either the T3b or T4 stage or primary Gleason pattern 5, or those who have more than four biopsies showing cancer or two or three high-risk features
Prostate Cancer Survival Rates and Statistics
Risk Assessment Tools
In addition to the NCCN guidelines, healthcare providers also use different risk assessment tools to aid clinical decision-making.
D’Amico Classification
The D’Amico classification was developed in 1998. It uses the following to estimate the risk of recurrence of prostate cancer:
PSA level
Gleason score
Tumor stage
Since it doesn’t take multiple risk factors into account, it may be less accurate in those with more than one risk factor.
Nomograms
Five prostate cancer nomograms can be used to assess risk and predict treatment outcomes. These are based on a person’s specific disease characteristics:5
Pre-radical prostatectomy nomogram is used to predict long-term results and the extent of cancer after removing the prostate gland and surrounding lymph nodes in people who have not yet begun treatment.
Post-radical prostatectomy nomogram is used after surgical intervention to predict cancer recurrence at 2, 5, 7, and 10 years after surgery. It is also used to determine the likelihood of survival in the 15 years following surgery.
Salvage radiation therapy nomogram is used to predict how effective salvage radiation therapy will be following radical prostatectomy if cancer recurs. It is also used to determine the probability of cancer control and the levels of undetectable PSA for 6 years following salvage therapy.
Risk of dying of prostate cancer in people with a rising PSA after radical prostatectomy nomogram. This estimates the risk of death if prostate cancer recurs following radical prostatectomy, signaled by rising PSA levels. It predicts the likelihood that a person initially treated with surgery will die of prostate cancer 5, 10, and 15 years from the time their PSA begins to rise.
Risk of high-grade cancer on a prostate biopsy nomogram is used to estimate the likelihood of having high-grade prostate cancer in people who have been considered eligible for prostate biopsy by a urologist. This tool does not apply to those who have already been diagnosed with prostate cancer.
USCF-CAPRA Score
The Cancer of the Prostate Risk Assessment (UCSF-CAPRA) estimates prostate cancer risk based on:6
Age at diagnosis
PSA at diagnosis
Gleason score of the biopsy
Clinical stage
Percentage of biopsy samples that have cancer
Each factor is assigned a score and then added up to calculate a final risk score. Thus, lower scores equal lower risks and vice versa.
Prostate screening is a personal decision that each individual must make for themselves. However, the American Urological Association (AUA) offers the following guidelines:7
Recommends against routine screening for people under 40
Does not recommend routine screening for people 40-54 at average risk
Shared decision-making between a person and their healthcare provider when they are between the ages of 55 and 69
Does not recommend routine screening for people over 70 or those with a life expectancy of less than 10-15 years
Genomic and Proteomic Tests
Genomic and proteomic tests can be used to better understand the possibility of cancer growth or spread. They look at both genes and proteins that are active inside prostate cancer cells to determine the risk. Some tests that are used include the Oncotype DX, Prolaris, ProMark, and Decipher.8
Recap
Risk assessment tools can help healthcare providers determine how your cancer might behave after treatment based on certain factors, like your age at diagnosis and your results from staging and screening tests.
Pre-Diagnosis Prediction Tools
In addition to risk assessment tools used to direct cancer treatment, there are also tools used to predict the likelihood that a biopsy will find prostate cancer. These tools help prevent overdiagnosis and unnecessary biopsy procedures.
Prostate Cancer Prevention Trial (PCPT) Risk Calculator
The Prostate Cancer Prevention Trial Risk Calculator was developed to help clinicians decide whether a biopsy is needed. It takes into account many clinical factors, including:9
PSA level
Exam results
Age
Race
Family history
Biopsy history
The results of the calculator may not apply to all individuals. Clinicians should only use it for those who:
Are 55 or older
Haven’t been diagnosed with prostate cancer in the past
Have results from a PSA or DRE that are less than 1 year old
Prostate Biopsy Collaborative Group (PBCG) Risk Calculator
The Prostate Biopsy Collaborative Group Risk Calculator (PBCG) is similar in nature to the PCPT in that it looks at a variety of factors to determine candidacy for a biopsy. Thus, it can help to reduce unnecessary biopsies. However, this and the PCPT calculators have shown disparities in results across different race groups.10
Prostate cancer treatment is approached with such consideration because the 5-year relative survival rate of all stages combined is high at 98%. Therefore, experts consider some treatment options unnecessary for survivability.11
Making Treatment Decisions
Prostate cancer is easily manageable, especially in the early stages. However, before undergoing treatment, you may want to discuss options with your healthcare provider so that you're not enduring unnecessary procedures.
If you are the type of person who can wait and see, active surveillance or watchful waiting may be a good option before undergoing treatment. It’s also important to consider the type of treatment and how well you can handle it. Radiation therapy may be a good option for those who don’t want to or can’t have surgery.
You should also consider treatment side effects, especially if you are in a low-risk group. Some side effects such as incontinence, impotence, and bowel issues may arise.12 Knowing how much time you’re willing to spend in treatment or recovery will also help you and your healthcare provider decide which treatment is best for you.
How Prostate Cancer Treatment Affects Longevity
Summary
Prostate cancer has an extremely high survivability rate. That's why healthcare providers approach screening, diagnosis, and treatment with such care.
Pre-diagnosis prediction tools can help your healthcare provider determine if you are a good candidate for screening tests. After a cancer diagnosis, numerous tests are used to stage cancer and predict your cancer risk. These all aid in narrowing down which treatment options might be best for you.





Post comments