
By Heidi Moawad, MD
Medically reviewed by Yaw Boachie-Adjei, MD
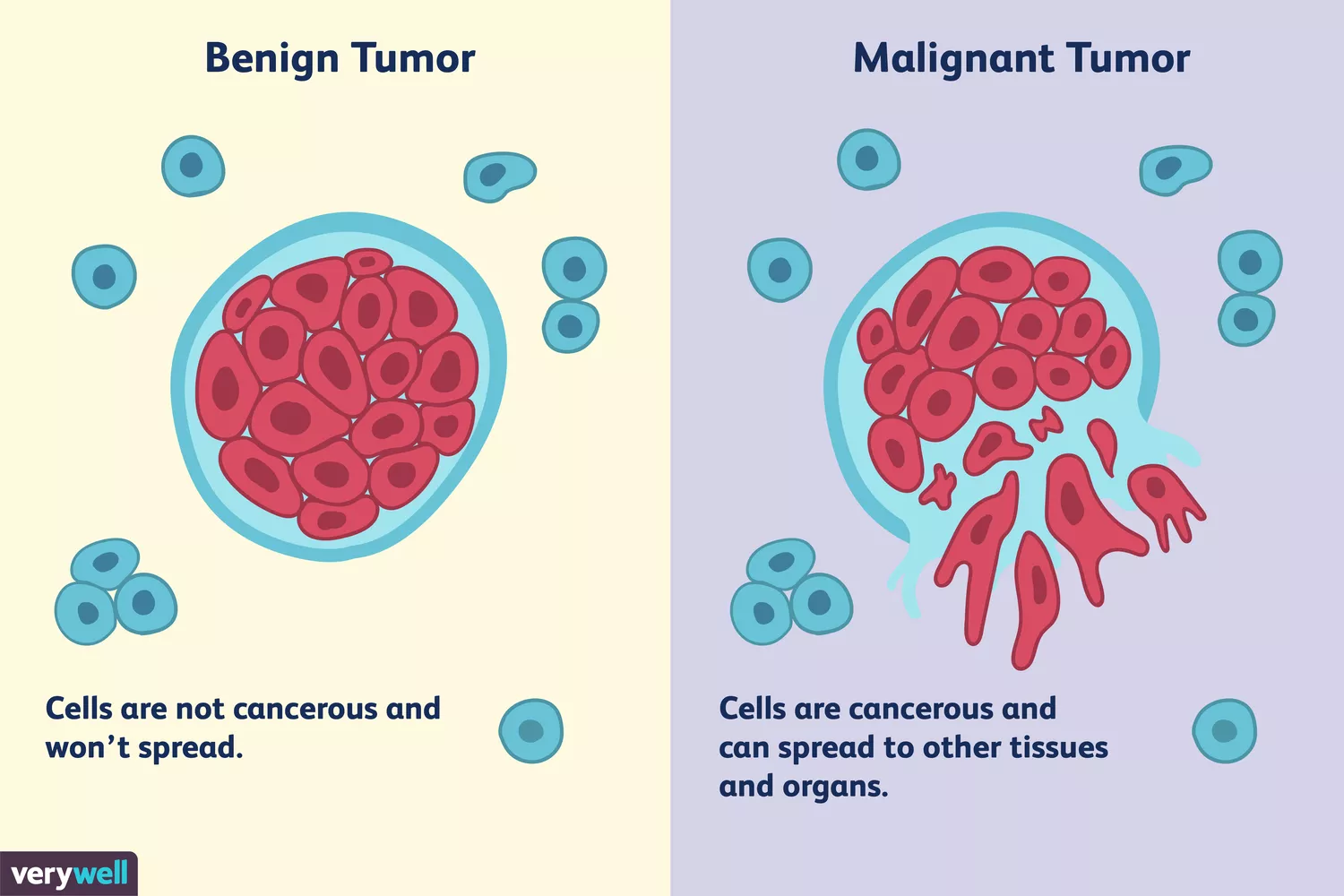
Tenosynovial giant cell tumors are benign (not dangerous), slow-growing tumors that affect joints in the fingers, hands, arms, shoulders, or legs. These tumors are relativity common, particularly in the hands and fingers. They are also called giant cell tumors of the tendon sheath or fibrous histiocytoma of the tendon sheath.1
Joints are the areas of your body that bend. They are composed of bones, cartilage, and muscles, which are held together with flexible tendons and ligaments. Synovial fluid lubricates the joints; it is produced by the synovium, a thin layer of tissue lining most joints. Tendon sheaths have a similar tissue layer called the tenosynovium. Tenosynovial giant cell tumors are growths caused by the thickening of the tenosynovium.
Verywell / JR Bee
Symptoms
Tenosynovial giant cell tumors typically affect people between ages 20 and 40, but they can occur at any age. Most people only have one tumor, but it is possible to have more than one. Symptoms generally begin gradually and slowly worsen over time.1
These tumors may cause swelling, enlargement, or visible growth. For example, the soft padded area between the joints in one of your fingers may appear enlarged if you have a tenosynovial giant cell tumor.
Tenosynovial giant cell tumors are described as firm in texture and are not tender to the touch. The skin around them may move a bit, but the tumors themselves are generally held to the structures beneath them, so you can’t change their shape, location, or appearance by moving, pushing, or squeezing them. These tumors generally range in size between one to four centimeters. Tumors that grow in larger joints are generally larger than tumors that grow in small joints.
The growths can also cause pain, discomfort, or joint stiffness. You may experience a decreased ability to move the affected area due to the swelling. The tumor can also press on a nerve, causing numbness or tingling, which may come and go.1
Sometimes, tenosynovial giant cell tumors can press on nearby bone, causing the bone around them to gradually erode (wither away). This can eventually lead to long-term consequences, such as bone fractures. But the tumors do not spread to other areas of the body and they are not life-threatening.
Rarely, tenosynovial giant cell tumors are completely asymptomatic (don’t cause symptoms) and may be incidentally discovered when an X-ray or another imaging test is done for an unrelated reason.
Causes
It is not clear why some people develop tenosynovial giant cell tumors. There are no recognized risk factors and there is not a hereditary cause.
There have been some theories regarding why they develop, including overgrowth of the soft tissue (non-bony area) of the joint due to chronic overuse or damage.
Some research suggests that the tumor cells have a mutation (abnormality in the gene of a cell) in chromosome 1, chromosome 2, chromosome 17, or a combination of these chromosomes. Translocations between chromosome 1 and chromosome 2 have been found. These are molecular changes in which two chromosomes erroneously “switch” genetic codes when cells are being formed.1
This genetic error does not mean that the tumor is inherited, however, because the mutation is only present in tumor cells, and not in all the cells of the body. The presence of a mutation in just this tiny area suggests that the generic error may develop during the healing of the joint.
Diagnosis
Your healthcare provider may be able to diagnose a tenosynovial giant cell tumor based only on your symptoms, its appearance, and the texture. Sometimes imaging tests or biopsies are needed, especially if there is a concern about another condition. You may also need diagnostic tests as part of your surgical planning if you are going to have your tumor removed.1
Imaging tests can help differentiate a tenosynovial giant cell tumor from other growths that produce similar swelling, such as fractures, joint injuries, infections, and inflammatory disease. These conditions tend to interfere with movement and cause more pain than tenosynovial giant cell tumors, but sometimes they can cause symptoms and an appearance that resembles that of tenosynovial giant cell tumors.
If there is any concern about the possibility of a malignant tumor, which would be prone to spread and may be life-threatening, you may need imaging tests and a biopsy.
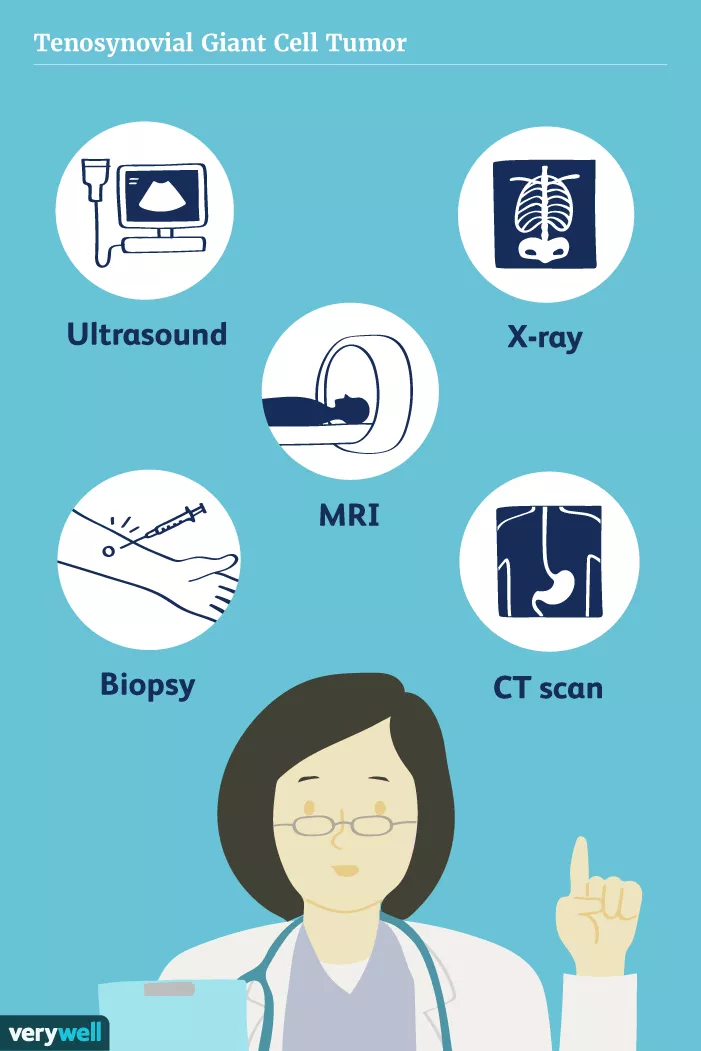
Tests you may need during your evaluation include:
X-Ray: An X-ray is an imaging test that only takes a few minutes and provides an immediate picture of your joint. X-rays of tenosynovial giant cell tumors typically show soft tissue swelling. If the erosion of the bone has occurred, this may show up on an X-ray as well.
Computerized Tomography (CT): A CT scan uses X-ray technology but is used to obtain more views of the joint, so it may provide more extensive visualization, especially for surgical planning. Like an X-ray, it can show areas of bone erosion and may also show soft tissue swelling.
Magnetic Resonance Imaging (MRI): An MRI is a highly technical test that uses magnets to produce an image. It takes longer than an X-ray and can also show evidence of soft tissue swelling and bone erosion, typically with more detail than an X-ray.
Ultrasound: An ultrasound is an imaging test typically used to evaluate fluid. If you have a growth that seems to be fluid-filled, then your healthcare provider might order an ultrasound, which can also identify a tenosynovial giant cell tumor.
Biopsy: If there is any concern that your tumor might be malignant, your healthcare provider might order a biopsy before deciding on your treatment plan. A biopsy is an interventional diagnostic procedure that involves the removal of a small piece of the growth for evaluation under a microscope. If your tumor is removed surgically, it is also likely to be examined under a microscope, although this wouldn’t technically be considered a biopsy.
Diagnosing by Types
A tenosynovial giant cell tumor has a characteristic appearance when examined under a microscope. These tumors are characterized by the presence of giant cells, which are large cells that typically contain more than one nuclei (the part of a cell that houses genetic material).
The major difference between the different types of giant cell tumors is that some are described as localized, while others are described as diffuse.1Localized lesions are encapsulated (enclosed) by protective collagen covering, while diffuse tumors are not. Tenosynovial giant cell tumors are usually localized, although some are diffuse. Typically, the collagen capsule is visualized on biopsy examination, which may provide some reassurance that the tumor has been completely removed. The diffuse tumors appear to grow as sheets and this pattern can be seen on microscopic examination
Pigmented Villonodular Synovitis
Pigmented villonodular synovitis (PVNS) is a diffuse giant cell tumor that is not classified as a tenosynovial giant cell tumor. PVNS is also called diffuse-type PVNS or diffuse-type giant cell tumor.2 Its appearance is very similar to that of tenosynovial giant cell tumor under a microscope. But PVNS growths are fast-growing and are more likely to interfere with movement and to spread within and around the joint. Because of their similar microscopic appearance, experts suggest that PVNS may be a type of tenosynovial giant cell tumor.
Treatment
Tenosynovial giant cell tumors can be removed, and you can use medication to manage the pain. Over-the-counter pain medications such as acetaminophen and non-steroidal anti-inflammatory agents (NSAIDs) such as naproxen and ibuprofen are usually effective for pain relief.
Surgical Removal
In general, it is recommended that tenosynovial giant cell tumors be treated surgically. They can usually be safely removed, but they have a tendency to recur. This is believed to be due to incomplete resection of the tumor. Overall, diffuse tumors are more likely to recur than localized tumors. Recurrence is not dangerous, but it can be uncomfortable. Some people may have repeated surgeries, but this can lead to scarring and stiffness of the joint.1
Medication
In August 2019, the U.S. Food and Drug Administration approved Turalio (pexidartinib) capsules.3 This drug is approved for use in adults with tenosynovial giant cell tumors that impact the quality of life and do not respond or improve with surgery. Turalio is recommended as the next step in these cases.
The option is a CSF1R inhibitor drug and is the first therapy approved for rare joint tumors.4
5 Sources
National Organization for Rare Disorders. Tenosynovial Giant Cell Tumor.
American Academy of Orthopaedic Surgeons. Pigmented Villonodular Synovitis.
Food and Drug Administration. FDA approves first therapy for rare joint tumor.
Wesolowski R, Sharma N, Reebel L, et al. Phase Ib study of the combination of pexidartinib (PLX3397), a CSF-1R inhibitor, and paclitaxel in patients with advanced solid tumors. Ther Adv Med Oncol. 2019;11:1758835919854238. doi:10.1177/1758835919854238
Haijun T, Yun L, Xinli Z, Zengming X. Treatment of tenosynovial giant-cell tumour types. The Lancet Oncology. 2019;20(8). doi:10.1016/s1470-2045(19)30419-x.

By Heidi Moawad, MD
Heidi Moawad is a neurologist and expert in the field of brain health and neurological disorders. Dr. Moawad regularly writes and edits health and career content for medical books and publications.





Post comments