
By Lynne Eldridge, MD
Medically reviewed by Susan Russell, MD
Neuroendocrine lung tumors, also known as pulmonary neuroendocrine carcinomas, are a spectrum of cancers that arise in neuroendocrine cells of the lungs. The majority are classified as small cell lung carcinomas (SCLCs), aggressive cancers that can affect neuroendocrine and other cell types. Others are carcinoid tumors, a rare and less-invasive form of cancer that only develops in neuroendocrine cells.1
Neuroendocrine lung tumors are relatively uncommon, accounting for only around 2% of all lung cancers.2 Still, the lung is the second most common place to find neuroendocrine cells after the gastrointestinal tract.1
The long-term prognosis for neuroendocrine tumors, as measured by the five-year survival rate, is generally good compared to other forms of lung cancer.
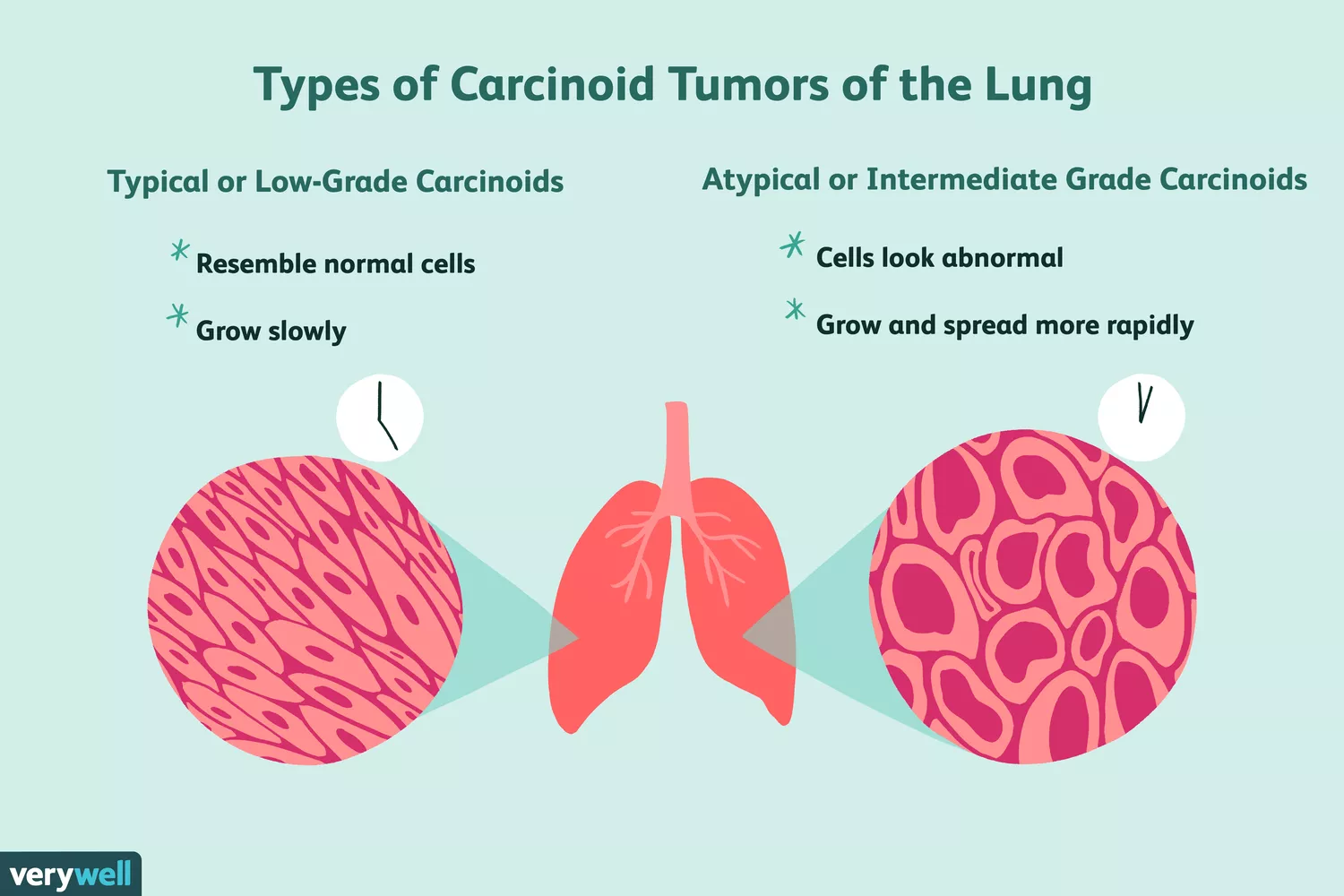
Illustration by Emily Roberts, Verywell
Types of Neuroendocrine Lung Tumors
Neuroendocrine cells are specialized cells responsible for repairing epithelial tissues that line the airways, intestines, and other surfaces of the body. They function both as neurons (nerve cells) and endocrine cells (responsible for the secretion of hormones).
There are four different types of neuroendocrine tumors (NETs) of the lungs. A NET can vary widely in terms of its cell type, aggressiveness, response to treatment, and prognosis. The one common feature among them is that they usually develop in the central airways, called the bronchi, located nearer to the middle of the chest.
Each type of neuroendocrine lung tumor is graded by its severity:
NET Type | Grade |
|---|---|
Typical carcinoid tumor | Low |
Atypical carcinoid tumor | Intermediate |
SCLC | High |
LCC | High |
Typical carcinoid tumors are a rare type of tumor that only develops in neuroendocrine cells. They are considered low-grade neuroendocrine tumors because they are generally slow-growing and less likely to spread (metastasize). Under the microscope, the cells look more like normal cells.
Atypical carcinoid tumors are related to typical carcinoid tumors but are far less common. These are considered intermediate-grade because the cells are less well-differentiated and tend to divide quicker.
Small cell lung cancer (SCLC) is the most common form of neuroendocrine tumor. It is considered high-grade because it is aggressive and more likely to spread. SCLC can cause cancer in neuroendocrine cells but also in cells of the submucosal lining of the airways.
Large cell lung carcinoma (LCC) is a type of non-small cell lung cancer (NSCLC) that only on rare occasions causes neuroendocrine lung cancer. It is differentiated from SCLC mainly by the size of its cells and is also considered high-grade due to its increased potential for metastasis.1
Neuroendocrine Lung Tumor Symptoms
Because neuroendocrine tumors tend to affect the large airways, they typically manifest with symptoms of airway obstruction as the tumor grows and begins to block air passages.
Common signs and symptoms of neuroendocrine lung tumors include:
Persistent cough
Wheezing
Shortness of breath
Hoarseness
Fatigue
Chest pain
Recurrent lung infections, such as bronchitis and pneumonia
Coughing up blood
As the disease progresses, people also often experience unexplained weight loss.
Hormonal Complications
Because of the role of neuroendocrine cells in producing hormones, NETs are known to secrete excessive amounts of hormones and similar-acting substances as the tumors grow and become more advanced. This can lead to a cluster of common and uncommon symptoms.
Neuroendocrine lung tumors of all types can secrete excessive amounts of adrenocorticotropic hormone (ACTH), leading to a condition known as Cushing's syndrome. Symptoms include weight gain, weakness, darkening of the skin, and excess hair growth on the body and face.3
Neuroendocrine lung tumors can sometimes also cause the excessive production of growth hormone (GH), leading to a condition known as acromegaly in which bones of the face, hands, and feet can grow abnormally.4
Carcinoid tumors, specifically, can excrete excess serotonin and prostaglandins when advanced. This can lead to a condition known as carcinoid syndrome, which manifests with facial flushing, facial lesions, diarrhea, rapid heart rate, and asthma-like symptoms.5
Neuroendocrine lung tumors can also cause hormonal imbalances that lead to hypercalcemia (abnormally high blood calcium), causing muscle cramps, confusion, irregular heartbeat, and other symptoms.6
Causes
On occasion, neuroendocrine cells can divide and grow abnormally and form cancerous tumors. Those that arise in the lungs are referred to as pulmonary neuroendocrine tumors. (Aside from the lungs, neuroendocrine tumors can also develop in the pancreas, colon, liver, rectum, ovaries, prostate gland, testes, breast, thyroid gland, thymus, pituitary gland, and adrenal glands.)1
While the causes of neuroendocrine tumors are unclear, several risk factors have been identified.
SCLC and LCC
SCLC and LCC are both strongly linked to cigarette smoking. In fact, up to 95% of people with these forms of lung cancer are either current or former smokers.
Environmental pollutants and occupational exposure to carcinogens (cancer-causing substances) are also common risk factors.
The average age of diagnosis of these cancers is around 70, with men being more affected than women.7
Carcinoid Tumors
The underlying cause is far less clear with carcinoid tumors. They are less commonly linked to smoking, environmental pollution, or occupational toxins.
These tumors can be found in young adults and even children. Women are more commonly affected than men, and more whites are affected than non-whites.
Genetics and family history are believed to play a part in the development of carcinoid tumors. Carcinoid tumors are associated with a number of genetic syndromes such as multiple endocrine neoplasia type 1 (MEN1).8
Studies suggest that as many as 10% of people with MEN1 will develop a carcinoid tumor, with one in six doing so before the age of 21. Children born to a parent with MEN1 have no less than a 50/50 chance of inheriting the syndrome.9
Diagnosis
The diagnosis of neuroendocrine tumors typically involves a combination of blood tests, imaging studies, and a lung biopsy.
Blood Tests
Blood tests cannot confirm neuroendocrine tumors, but they are included in the diagnostic process because they can help distinguish subtypes and, hence, the grade of the disease.
The Ki67 proliferation index is a blood marker test used to differentiate high-grade from low-grade tumors. It can also be used to estimate the likelihood of recurrence and severity.10
In addition to performing a general blood chemistry panel to check for hypercalcemia and other abnormalities, the healthcare provider may order blood tests to measure ACTH, growth hormone, and other hormone levels. Typically speaking, hormone levels tend to be excessively high when neuroendocrine lung cancer is advanced.
Imaging Studies
A chest X-ray is often the first test done when lung cancer is suspected, but carcinoid tumors are easily missed in 25% of cases.11 With lung cancer in general, chest X-rays tend to underperform and can miss as many as nine of every 10 malignancies in the earlier stages.12
If neuroendocrine cancer is suspected, your healthcare provider will more likely order other imaging studies:
Computed tomography (CT) scans take multiple X-ray images to create three-dimensional "slices" of inner organs and structures. For neuroendocrine cancer, both the lungs and abdomen would be scanned.
Magnetic resonance imaging (MRI) scans create highly detailed images, particularly of soft tissues, using powerful magnetic and radio waves.
Positron emission tomography (PET) scans use mild radioactive tracers to detect areas of increased metabolic activity (as occurs with cancer). This can help the healthcare provider see if the cancer is localized or has spread to other parts of the body.
Somatostatin receptor scintigraphy (SRS) is a newer procedure that uses a mild radioactive, hormone-like substance called octreotide that can bind to and identify carcinoid tumors specifically.
Lung Biopsy
A lung biopsy is considered the gold standard for a lung cancer diagnosis. There are several ways that a healthcare provider can obtain a sample of tissue for evaluation:
Bronchoscopy is a procedure in which a tube-like camera is fed through the mouth and into the bronchi to view the airways. During the procedure, a special attachment can be fed through the scope to obtain a tissue sample.
Endobronchial ultrasonography is a similar procedure in which a narrow ultrasound transducer is fed through the mouth to visualize the central airways and obtain tissue samples.
Fine-needle aspiration (FNA) involves the insertion of a hollow-core needle into the chest to extract a small sample of tumor tissue.
Laparoscopic surgery is a minimally invasive form of surgery in which "keyhole" incisions are made so that abnormal masses and lymph nodes can be removed using specialized operating equipment.
Open surgery is less commonly used to obtain biopsy samples unless there are medical complications that motivate its use.
Cancer Staging
Once neuroendocrine lung cancer is diagnosed, it is staged to characterize the severity of the disease, direct the appropriate treatment, and predict the likely outcome (prognosis).
LCC and carcinoid tumors are staged in the same way as non-small cell lung cancers, with five stages ranging from stage 0 to stage 4. The staging is based on the TNM classification system which characterizes the malignancy based on the size of the tumor (T), whether lymph nodes are involved (L), and whether the malignancy has metastasized (M). Stages 0, 1, 2, and 3A are considered early-stage lung cancer, whereas stages 3B and 4 are advanced.13
Small cell lung cancers are staged differently. Instead of five stages, there are two: limited-stage and extensive-stage. Limited-stage SCLC is confined to a certain part of the lung and has a better prognosis, while extensive-stage SCLC has spread and has a poor prognosis.
Treatment of High-Grade NETs
The treatment of neuroendocrine lung tumors can vary by the tumor type, cancer stage, tumor location, and the general health of the individual being treated.
The treatment of high-grade neuroendocrine tumors is no different than that of any other form of SCLC or LCC:
SCLC treatment may involve local treatments (surgery, radiation therapy, ablation therapies) and system treatments (chemotherapy, targeted therapies, immunotherapy).
LCC treatment may involve surgery, chemotherapy, radiation therapy, targeted therapy, immunotherapy, or a combination of these.
Treatment of Intermediate and Low-Grade NETs
The same cannot be said of low- to intermediate-grade carcinoid tumors, which do not respond to newer targeted therapies and immunotherapies for certain non-small cell lung cancers. Even chemotherapy and radiation therapy are not used in quite the same way with carcinoid tumors and have different degrees of efficacy.
With that said, carcinoid tumors are responsive to surgery and other medications not commonly used in lung cancer therapy.
Surgery
The prognosis of carcinoid tumors is much better than other types of lung cancer. When it's caught in the early stages, surgery can be curative.
With early-stage carcinoid tumors, lung cancer surgery is the treatment of choice. Depending on the size of the tumor, a healthcare provider may recommend one of the following:
Wedge resection, in which a wedge of lung tissue is removed
Lobectomy, in which a lobe of a lung is removed
Pneumonectomy, in which an entire lung is removed
Surrounding lymph nodes may also be resected (removed) as they often contain cancer cells. These include lymph nodes situated where the bronchi enter the lungs (hilar lymph nodes) or lymph nodes situated between the lungs (mediastinal lymph nodes).
As drastic as these surgeries sound, many people are able to live full, active lives with only one lung or a portion of a lung.
Afinitor (Everolimus)
The treatment of carcinoid tumors is more challenging once the disease is advanced. In 2016, a biologic drug called Afinitor (everolimus) was approved for the first-line treatment for lung carcinoid tumors and has been shown to significantly slow the progression of even advanced malignancies.
Afinitor works by inhibiting a protein called mammalian target of rapamycin (mTOR), which regulates cell growth.
This drug is recommended for progressive, inoperable carcinoid tumors that do not secrete hormone-like substances (a.k.a. non-functional carcinoids).14 Afinitor has been found to decrease the progression of both typical and atypical carcinoids as well as extend survival times.15
Afinitor is taken as a daily pill but may causes side effects in at least 30% of users, including stomach inflammation, diarrhea, nausea, fever, rash, and hives.14
Somatostatin Analogues
Somatostatin analogs are a class of drugs that have long been used to treat gastrointestinal carcinoid tumors, both functional and non-functional. They are now recommended as the first-line treatment for people with indolent (slow-growing) somatostatin receptor-positive carcinoid lung tumors.
Lab pathologists can determine if a carcinoid tumor has somatostatin receptors by exposing biopsied tissues to specialized stains. If it does, it means that the tumor has attachment points onto which the drug molecule can latch.
Somatostatin analogs cannot cure carcinoid tumors but can temporarily reduce their size along with accompanying symptoms. The somatostatin analogs commonly used in the treatment of carcinoid lung tumors include:
Sandostatin (octreotide)
Signifor (pasireotide)
Somatuline (lanreotide)16
Chemotherapy and Radiation Therapy
Carcinoid tumors are not very responsive to standard chemotherapy drugs. Even so, chemotherapy may be used for tumors that are not responsive to other forms of therapy, especially those that have a high Ki67 proliferation index.13
Radiation therapy may be an option for early-stage tumors when surgery is not possible. Specialized techniques such as stereotactic body radiosurgery (SBRT) deliver high doses of radiation to a focused area of tissue and can sometimes provide similar results to those attained with surgery.13
Radioactive drugs, such as radioactive octreotide used in somatostatin receptor scintigraphy, may also be used in higher doses to treat carcinoid tumors. This approach is considered experimental but has proven effective for some people with advanced carcinoid tumors.17
On the Horizon
Peptide receptor radionuclide therapy (PPRT) is a new therapeutic application of nuclear medicine currently approved for the treatment of advanced neuroendocrine tumors of the gastrointestinal system that will be likely used in the near future also in the treatment of advanced neuroendocrine tumors of the lung. PRRT could be described as a kind of systemic radiotherapy. 177Lu-DOTATATE and 90Y-DOTATOC are the two representative compounds of PRRT and contain Lutetium-177 and Yttrium-90, respectively.18
Since relatively few studies have looked at the best treatment options for advanced carcinoid tumors, there is currently no standardized approach for them.
NET Type | Treatment Options |
|---|---|
Small cell lung cancer | • Chemotherapy |
Large cell lung carcinoma | • Surgery |
Carcinoid tumors
| • Surgery |
Prognosis
The prognosis for neuroendocrine tumors caused by SCLC and LCC is historically poor.19 By contrast, low- and intermediate-grade carcinoid tumors tend the have better outcomes and a far lower risk of metastases.20
5-Year Survival Rates by Tumor Type | |
|---|---|
Typical carcinoid tumor | 89% |
Atypical carcinoid tumor | 58% |
Limited-stage SCLC | 27% |
LCC | 13% |
Extensive-stage SCLC | 5% |
Despite the fact that SCLC and LCC have poorer prognoses overall, improved diagnostics and treatments are extending survival times every year.
21 Sources
Rekhtman N. Neuroendocrine tumors of the lung: An update. Arch Pathol Lab Med. 2010 Nov;134(11):1628-38.
Oronsky B, Ma PC, Morgensztern D, Carter CA. Nothing but NET: A review of neuroendocrine tumors and carcinomas. Neoplasia. 2017;19(12):991-1002. doi:10.1016/j.neo.2017.09.002
Zainal A, Akinsola O, Rajamani K. Cushing syndrome secondary to primary neuroendocrine lung carcinoma. Case Rep Endocrinol. 2019;2019:1989260. doi:10.1155/2019/1989260
Jawiarczyk-Przybyłowska A, Wojtczak B, Whitworth J, et al. Acromegaly associated with GIST, non-small cell lung carcinoma, clear cell renal carcinoma, multiple myeloma, medulla oblongata tumour, adrenal adenoma, and follicular thyroid nodules. Endokrynol Pol. 2019;70(2):213-7. doi:10.5603/EP.a2019.0005
Gade AK, Olariu E, Douthit NT. Carcinoid syndrome: A review. Cureus. 2020;12(3):e7186. doi:10.7759/cureus.7186
Kanaji N, Watanabe N, Kita N, et al. Paraneoplastic syndromes associated with lung cancer. World J Clin Oncol. 2014;5(3):197-223. doi:10.5306/wjco.v5.i3.197
National Organization of Rare Disease. Small cell lung cancer.
American Cancer Society. Risk factors for lung carcinoid tumors.
Kamilaris CDC, Stratakis CA. Multiple endocrine neoplasia type 1 (MEN1): An update and the significance of early genetic and clinical diagnosis. Front Endocrinol (Lausanne). 2019;10:339. doi:10.3389/fendo.2019.00339
Dermawan JKT, Farver CF. The Role of Histologic Grading and Ki-67 Index in Predicting Outcomes in Pulmonary Carcinoid Tumors. Am J Surg Pathol. 2020 Feb;44(2):224-231. doi: 10.1097/PAS.0000000000001358
Demirci I, Herold S, Kopp A, et al. Overdiagnosis of a typical carcinoid tumor as an adenocarcinoma of the lung: a case report and review of the literature. World J Surg Onc. 2012;10:19. doi:0.1186/1477-7819-10-19
Del Ciello A, Franchi P, Contegiacomo A, Cicchetti G, Bonomo L, Larici AR. Missed lung cancer: when, where, and why?. Diagn Interv Radiol. 2017;23(2):118-26. doi:10.5152/dir.2016.16187
Kaifi JT, Kayser G, Ruf J, Passlick B. The diagnosis and treatment of bronchopulmonary carcinoid. Dtsch Arztebl Int. 2015 Jul;112(27-28):479-85. doi:10.3238/arztebl.2015.0479
Novartis. Afinitor (everolimus) tablets for oral administration.
Fazio N, Buzzoni R, Delle Fave G, et al. Everolimus in advanced, progressive, well-differentiated, non-functional neuroendocrine tumors: RADIANT-4 lung subgroup analysis. Cancer Sci. 2018;109(1):174-81. doi:10.1111/cas.13427
Gomes-Porras M, Cárdenas-Salas J, Álvarez-Escolá C. Somatostatin analogs in clinical practice: A review. Int J Mol Sci. 2020;21(5):233-45. doi:10.3390/ijms21051682
Tsoukalas N, Baxevanos P, Aravantinou-Fatorou E, et al. Advances on systemic treatment for lung neuroendocrine neoplasms. Ann Transl Med. 2018;6(8):146. doi:10.21037/atm.2018.04.03
National Cancer Institute. FDA Approves New Treatment for Certain Neuroendocrine Tumors.
Lu T, Yang X, Huang Y, et al. Trends in the incidence, treatment, and survival of patients with lung cancer in the last four decades. Cancer Manag Res. 2019;11:943-53. doi:10.2147/CMAR.S187317
Ramirez RA, Beyer DT, Diebold AE, et al. Prognostic factors in typical and atypical pulmonary carcinoids. Ochsner J. 2017;17(4):335-40.
US Preventive Services Task Force. Screening for Lung Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2021;325(10):962–970. doi:10.1001/jama.2021.1117

By Lynne Eldridge, MD
Lynne Eldrige, MD, is a lung cancer physician, patient advocate, and award-winning author of "Avoiding Cancer One Day at a Time."






Post comments