
by European Alliance of Associations for Rheumatology, EULAR
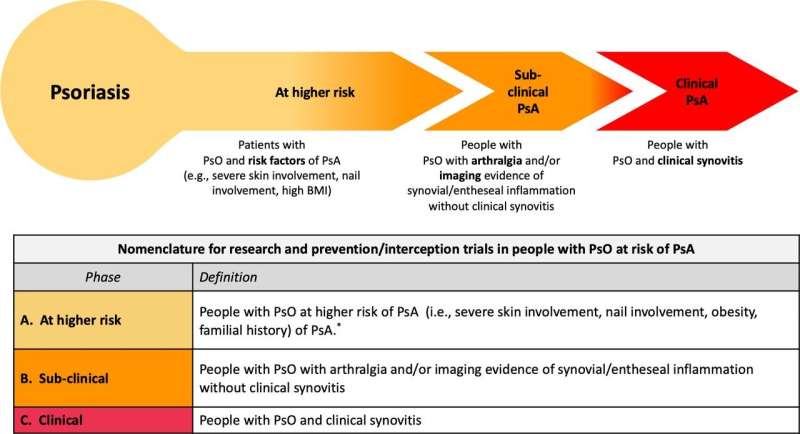
Proposed nomenclature for the transition from PsO to PsA for clinical trials of PsA prevention. A simple three-stage scheme for progression from at risk of PsA to frank PsA. It is acknowledged that onset may be variable and could occur quickly in some subjects, for example, after trauma or following infection with a reactive arthritis type onset. Although arrows imply directionality and inevitable progression, it is acknowledged that some subjects may have spontaneous resolution of PsA and that subjects with arthralgia may regress and that strategies in at-risk people, for example, weight loss in obesity may lead to reduction of risk. This scheme recognizes the importance of enthesitis in pathophysiology but for trials of interception suggest the use of synovitis development as an outcome measure since this was by far the most common manifestation of early disease from the accompanying systematic literature reviews. *Role of immunogenetics awaits definition. BMI, body mass index; PsA, psoriatic arthritis; PsO, psoriasis. Credit: Annals of the Rheumatic Diseases (2023). DOI: 10.1136/ard-2023-224148
The transition from psoriasis to psoriatic arthritis (PsA)—and the early diagnosis of PsA—is of considerable scientific and clinical interest. People typically have psoriatic skin disease for a decade or more before they begin to experience the joint involvement of PsA. Understanding more about the natural history and trajectory of this disease will help in the future prevention of PsA, as well as shed more light on possible risk factors and predictors.
The new EULAR points-to-consider were developed by a multidisciplinary task force of 30 members from 13 European countries, with health care professionals from rheumatology and dermatology, as well as methodologists and patient research partners. The work was completed in line with EULAR standardized operating procedures. All information included in the final paper, published in the Annals of the Rheumatic Diseases, was based on two systematic literature reviews plus expert consensus.
Overall, five overarching principles and 10 points-to-consider were formulated. The principles acknowledge that people with psoriasis may develop PsA at different times—or not at all—and highlight that there is a need for close collaboration between dermatologists and rheumatologists, although the rheumatologist has a key role in PsA diagnosis and management. They also stress that being able to identify risk factors for PsA may influence therapy choices in people with psoriasis, especially since certain systemic treatments for psoriasis may reduce the risk of transition to PsA.
The points-to-consider highlight arthralgia (joint pain) and abnormalities seen on ultrasound or MRI (magnetic resonance imaging) as key elements of subclinical PsA that can potentially be used as short-term predictors of who will go on to develop PsA. This also makes these elements useful to help design clinical trials looking at PsA interception and prevention. Traditional risk factors for PsA development such as psoriasis severity, obesity and nail involvement may represent more long-term disease predictors. As such, these are felt to be less useful for short-term trials investigating the transition from psoriasis to PsA.
The task force also proposed some standard naming for three distinct stages in PsA development. First, people with psoriasis at higher risk of PsA, then people with subclinical PsA, and then people with clinical PsA. This is important, as it has been shown in other inflammatory rheumatic musculoskeletal diseases that clinical onset is preceded by a preclinical phase where a person has arthralgia and immunological or imaging abnormalities, in the absence of a clinical diagnosis. The task force also proposed a definition for early psoriatic arthritis based on the development of joint swelling as a clinical outcome measure for trials of PsA prevention.
EULAR hopes this publication will help to define the clinical and imaging features of people with psoriasis who should raise clinical suspicion for progression to PsA. They also hope it can be used to identify people who could benefit from a therapeutic intervention to delay or prevent PsA. In the meantime, people with psoriasis should be informed about the risk of developing PsA and encouraged to report their symptoms to facilitate early PsA recognition.
More information: Alen Zabotti et al, EULAR points to consider for the definition of clinical and imaging features suspicious for progression from psoriasis to psoriatic arthritis, Annals of the Rheumatic Diseases (2023). DOI: 10.1136/ard-2023-224148
Journal information: Annals of the Rheumatic Diseases
Provided by European Alliance of Associations for Rheumatology, EULAR






Post comments