
By Richard N. Fogoros, MD
Medically reviewed by Jeffrey S. Lander, MD
Most cardiologists and lipid experts have long subscribed to the “cholesterol hypothesis” (also called “lipid hypothesis”). The cholesterol hypothesis, simply stated, is that an elevated blood level of LDL cholesterol is a direct cause of atherosclerosis, a progressive disease where arteries become clogged with plaque.
As a result, the medical community’s consensus has been to help people reduce LDL cholesterol levels to lower the risk of atherosclerotic cardiovascular disease.
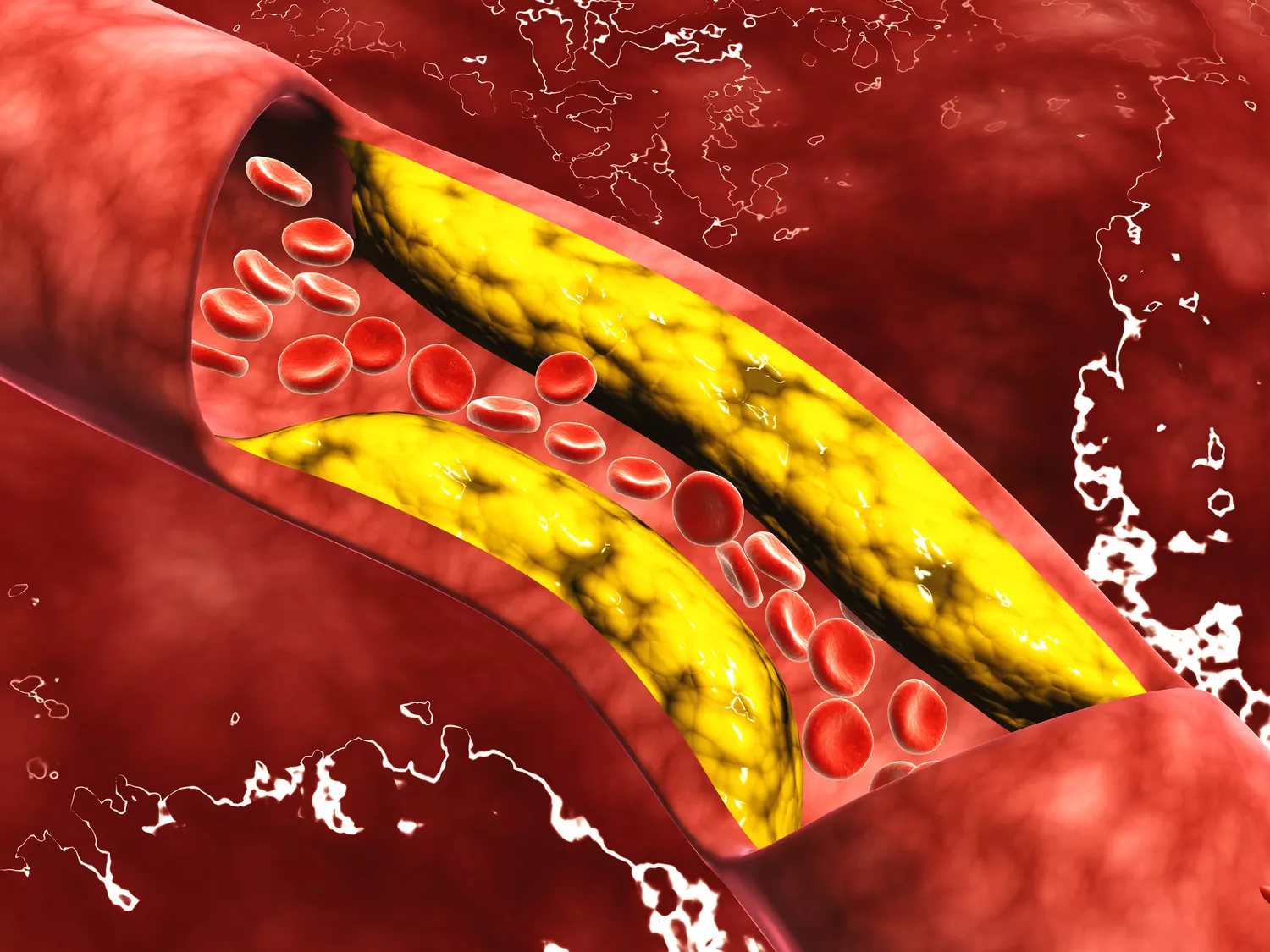
Stocktrek Images/Getty Images
However, more recently, experts have been questioning the cholesterol hypothesis. This article explains the theory, its implications, and factors besides cholesterol that researchers are considering.
What Is the Cholesterol Hypothesis?
The cholesterol hypothesis is based on several observations:
Cholesterol and plaque: Pathologists showed a long time ago that cholesterol deposits are a significant component of atherosclerotic plaques.
Cholesterol and heart disease: Epidemiological studies—particularly the Framingham Heart Study—showed that people with high blood cholesterol levels have a significantly higher risk of cardiovascular disease.1
Cholesterol-lowering medication: In the 1990s, randomized clinical trials demonstrated the value of cholesterol-lowering medication. In those trials, select people with elevated cholesterol levels achieved improved clinical outcomes by reducing their LDL cholesterol levels with statin drugs. For many experts, these trials proved the cholesterol hypothesis once and for all.1
Recap
The cholesterol hypothesis is that high levels of cholesterol can lead to atherosclerotic heart disease and that lowering cholesterol can improve outcomes.
Guidelines
These studies resulted in guidelines encouraging people to reduce their risk of heart disease by lowering their cholesterol. As a result, in 1977, the U.S. Senate Select Committee on Nutrition and Human Needs formally recommended that Americans reduce their fat intake—especially saturated fat.2
American Heart Association Recommendations
Currently, the American Heart Association recommends dietary modifications to reduce the risk of cardiovascular disease. Specifically, they recommend reducing saturated fat intake and replacing it with unsaturated fat, especially polyunsaturated fat.3
For decades, experts urged people to alter their diets to reduce cholesterol levels. In addition, pharmaceutical companies spent billions of dollars developing drugs for lowering cholesterol.
The cholesterol hypothesis became ingrained among healthcare providers, the medical community, and the population at large.
The Problem
Many lipid experts and cardiologists are now questioning whether the cholesterol hypothesis is true after all. That’s because trials have failed to show a clinical benefit when using drugs other than statins to reduce cholesterol levels.
The problem is that if the cholesterol hypothesis were true, it should not matter which drugs were used to reduce cholesterol; any method of lowering cholesterol should theoretically improve clinical outcomes. But that has not been shown.
Non-Statin Therapies
Some studies found substantially lowered LDL cholesterol levels with non-statin therapies. However, they did not show improved cardiovascular outcomes.
Treatments used in these studies included:
Niacin
Fibrates
Ezetimibe
Bile acid sequestrants4
CETP inhibitors5
Hormone replacement therapy in post-menopausal people6
Indeed, despite improved cholesterol levels in some of these trials, a substantially worse cardiovascular outcome was seen with treatment.7
Statins
In general, of the cholesterol-lowering trials conducted so far, it is fair to say that reducing cholesterol levels with statins seems to improve cardiovascular outcomes. However, reducing them with other interventions does not.
This result suggests that the benefits of cholesterol-lowering seen with statin therapy are specific to the statins themselves. For this reason, the cholesterol hypothesis, at least in its classic form, is now being questioned.
Statins represent a special case when it comes to cholesterol-lowering therapy. Statins have many effects on the cardiovascular system.
In addition to reducing cholesterol levels, they may also:
Have anti-inflammatory properties8
Fight infections9
Lower blood pressure10
These other effects stabilize atherosclerotic plaques and could explain much of the clinical benefit seen with statins.
Drugs that lower cholesterol without having these other plaque-stabilizing characteristics seem not to result in this kind of benefit. Therefore, it is reasonable to postulate that statins do not improve cardiovascular risk only by reducing cholesterol levels. Instead, they might be doing so through these other effects.
PCSK9 Inhibitors
Trials found that when a PCSK9 inhibitor (an anti-cholesterol drug) is added to maximal statin therapy, it resulted in:
Ultra-low LDL levels
Improved clinical outcomes
In the PCSK9i trials (e.g., the FOURIER trial) both cohorts were on statins, and the cohort that had PCSK9i in addition to statin showed benefit above and beyond the other group that was also on a statin but not on a PCSK9i.11
Impact on Guidelines
The growing doubts about the cholesterol hypothesis became public in 2013, with the American Heart Association’s new guidelines on cholesterol treatment. In a significant break with prior cholesterol guidelines, the 2013 version abandoned the recommendation to reduce LDL cholesterol to specific target levels.12
Instead, the guidelines focused on deciding which people should treat their condition with statins. In fact, for most people, these guidelines generally recommend against using non-statin drugs to lower cholesterol.
These guidelines created tremendous controversy within the cardiology community.13
Recap
Experts are questioning the cholesterol hypothesis. That’s because studies have found that non-statin therapies alone have not improved outcomes. It has been considered that statins’ other effects on the body may play a role in their clinical benefit.
Potential Solutions
While cholesterol has a role in the formation of atherosclerotic plaques, other factors are also at play.
Some questions experts are considering include:
Why do some people with high LDL cholesterol levels never develop significant atherosclerosis?
Why do some people with “normal” LDL cholesterol levels have widespread cholesterol-filled atherosclerotic plaques?
Why does lowering LDL cholesterol levels with one drug improve outcomes, while lowering LDL levels with another drug does not?14
Experts have different ideas for how to move forward. Some think it’s time to abandon the cholesterol hypothesis altogether, while others believe the medical community should revise it.15
Trials looking at diet to reduce cholesterol have shown an improvement in clinical outcomes.
Abandoning the Cholesterol Hypothesis
Those in this camp believe that if high LDL cholesterol was a direct cause of atherosclerosis, then lowering LDL cholesterol levels by any method should improve cardiovascular outcomes. They suggest that after the cholesterol-lowering clinical trials using many different cholesterol-reducing agents did not find those expected results, the cholesterol hypothesis must be wrong.
Many healthcare providers and a fair number of cholesterol experts seem to be ready to accept this line of thinking and abandon the cholesterol hypothesis altogether.16
Revising the Cholesterol Hypothesis
Other experts—likely the majority—still agree with the idea that cholesterol levels are important. They hold this view because no matter how you cut it when it comes to atherosclerotic cardiovascular disease, cholesterol does matter.16
Atherosclerotic plaques are loaded with cholesterol. There is also strong evidence that the cholesterol that ends up in the plaques is delivered there by LDL particles.17
Reducing cholesterol may shrink plaque. There is at least some evidence that when you lower LDL cholesterol in the blood to very low levels, you can begin to reverse the atherosclerotic process—and make plaques shrink.17
Given this line of evidence, it seems premature to assert that cholesterol levels do not matter.
Any hypothesis is a working model. As you learn more, you change the model. By this reasoning, it makes sense for the cholesterol hypothesis to be revised.
The Role of Lipoproteins
It is now quite apparent that it’s just not cholesterol blood levels alone that are important. It’s also the type and behavior of the lipoprotein particles that carry the cholesterol.
Lipoprotein
Lipoproteins help transport cholesterol and triglycerides (a form of fat in the body used to store energy) in blood.
In particular, how and when various lipoprotein particles interact with the endothelium of the blood vessels impacts how the blood vessels promote or hamper plaque formation.
Endothelium
The endothelium is the inner cell lining of the body’s arteries. It allows for proper blood vessel dilation and constriction, impacts blood pressure, protects the body against toxic substances, and regulates blood clotting.
Scientists are rapidly learning more about the various lipoprotein particles and what influences how they behave.
For instance:
Size: Some are small, dense particles, and some are big, “fluffy” particles. The small particles are much more likely to produce atherosclerosis than the larger particles.
Oxidized: Oxidized LDL particles are relatively toxic to cardiovascular health. These particles are more likely to worsen atherosclerosis.
The makeup and the “behavior” of LDL particles seem to be influenced by activity levels, diet, hormone levels, and medications.
At some point, there will likely be a new, revised cholesterol hypothesis that considers new understandings about the behaviors of LDL, HDL, and other lipoproteins.
New ways of changing the behaviors of these lipoproteins may help reduce cardiovascular disease.
Recap
In addition to cholesterol, other factors, like the behavior of lipoproteins, play a role in the development of atherosclerotic plaques.
Summary
The classic cholesterol hypothesis is that the lower your cholesterol levels, the lower your risk for cardiovascular disease. But, recently, more experts are suggesting that the hypothesis is too simplistic. That’s because the range of results from cholesterol-lowering trials is inconsistent.
Namely, some studies have found that lowering cholesterol alone does not consistently improve outcomes. Some studies indicate that statins’ additional benefits may play a role in why they work.
Experts are in an uncomfortable place where the hypothesis and associated guidelines may need modification. There is not a replacement yet.
Sources
Mahmood SS, Levy D, Vasan RS, Wang TJ. The Framingham Heart Study and the epidemiology of cardiovascular disease: a historical perspective. Lancet. 2014;383(9921):999-1008. doi:10.1016/S0140-6736(13)61752-3
Senate Select Committee on Nutrition and Human Needs. Dietary goals for the United States, 2nd edition.
Sacks FM, Lichtenstein AH, Wu JHY, et al. Dietary fats and cardiovascular disease: a presidential advisory from the American Heart Association. Circulation. 2017;136(3):e1-e23. doi:10.1161/CIR.0000000000000510
Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082-e1143. doi:10.1161/CIR.0000000000000625
Nicholls SJ, Ruotolo G, Brewer HB, et al. Cholesterol efflux capacity and pre-beta-1 HDL concentrations are increased in dyslipidemic patients treated with evacetrapib. J Am Coll Cardiol. 2015;66(20):2201-2210. doi:10.1016/j.jacc.2015.09.013
Cífková R, Krajčoviechová A. Dyslipidemia and cardiovascular disease in women. Curr Cardiol Rep. 2015;17(7):609. doi:10.1007/s11886-015-0609-5
Lloyd-Jones DM, Morris PB, Ballantyne CM, et al. 2022 ACC expert consensus decision pathway on the role of nonstatin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk: a report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2022;80(14):1366-1418. doi:10.1016/j.jacc.2022.07.006
Zahedipour F, Guest PC, Majeed M, Al-Rasadi K, Jamialahmadi T, Sahebkar A. Multiplex testing of the effect of statins on disease severity risk in COVID-19 cases. Methods Mol Biol. 2022;2511:273-284. doi:10.1007/978-1-0716-2395-4_20
Liang B, Yang ST, Wei KK, et al. Statin use and mortality among patients hospitalized with sepsis: a retrospective cohort study within southern California, 2008-2018. Crit Care Res Pract. 2022;2022:7127531. doi:10.1155/2022/7127531
Alghamdi J, Alqadi A, Alharf A, et al. Blood pressure-lowering activity of statins: a systematic literature review and meta-analysis of placebo-randomized controlled trials. Eur J Clin Pharmacol. 2020;76(12):1745-1754. doi:10.1007/s00228-020-02965-2
Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713-1722. doi:10.1056/NEJMoa1615664
Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 Pt B):2889-2934. doi:10.1016/j.jacc.2013.11.002
Ades PA. A controversial step forward: a commentary on the 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults. Coron Artery Dis. 2014;25(4):360-363. doi:10.1097/MCA.0000000000000086
Ravnskov U, de Lorgeril M, Diamond DM, et al. LDL-C does not cause cardiovascular disease: a comprehensive review of the current literature. Expert Rev Clin Pharmacol. 2018;11(10):959-970. doi:10.1080/17512433.2018.1519391
DuBroff R. A reappraisal of the lipid hypothesis. Am J Med. 2018;131(9):993-997. doi:10.1016/j.amjmed.2018.04.027
DuBroff R. Cholesterol paradox: a correlate does not a surrogate make. Evid Based Med. 2017;22(1):15-19. doi:10.1136/ebmed-2016-110602
Goldstein JL, Brown MS. A century of cholesterol and coronaries: from plaques to genes to statins. Cell. 2015;161(1):161-172. doi:10.1016/j.cell.2015.01.036
Additional Reading
Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082-e1143. doi:10.1161/CIR.0000000000000625

By Richard N. Fogoros, MD
Richard N. Fogoros, MD, is a retired professor of medicine and board-certified in internal medicine, clinical cardiology, and clinical electrophysiology





Post comments