
by University of Bergen
Pregnancy leads to a lot of radical changes within the body. The entire cardiovascular system reorganizes itself to sustain life for a second person inside the womb. The heart starts beating faster, and the total amount of blood in the body doubles. Mothers grow an entirely new organ, the placenta, to feed and protect the growing baby. All of this is normal, healthy, and safe.
Until it's not. Around five to ten percent of people develop a problem with their cardiovascular system during pregnancy in response to these physiological changes and/or problems with the placenta, like "preeclampsia." The umbrella term for these problems is "hypertensive disorders of pregnancy" (HDP).
Some disorders are rather benign, like high blood pressure during pregnancy. Others are true emergencies, including liver failure, kidney failure, and seizures. It is thought that all of these disorders share a common cause, only varying in the severity of symptoms.
Sage Wyatt, Ph.D.-candidate at the Department of Global Public Health and Primary Care, University of Bergen, is a part of the HealthierWomen Project (led by Rolv Skjærven) at the University of Bergen.
The purpose of the project is to look into women's lifetime reproductive history and later health. Other colleagues, including Associate Professor Liv Kvalvik, have already published work on predicting CVD death from history of pregnancy complications at age 40. Wyatt has specifically explored how HDP can predict stroke and heart attack in old age.
While with proper medical care, it is extremely rare for people with hypertensive disorders of pregnancy to die during childbirth, many go on to suffer from heart disease many decades later. In other words, the challenging time during pregnancy can offer a snapshot into the future.
"It has been hypothesized that HDP is indicative of a chronic underlying CVD that manifests during the 'stress test' of pregnancy," Wyatt explains.
Almost a ten-fold increased risk
Before now, data scientists researching hypertensive disorders of pregnancy have focused on the relationship between just one pregnancy with HDP and the long-term risk of heart attack and stroke.
"But a pregnant person isn't just one pregnancy. They are a unique individual, with a unique lifetime history of hypertensive disorders of pregnancy," says Wyatt.
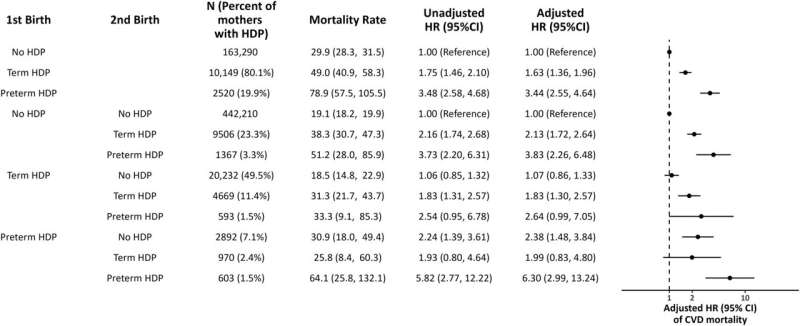
With the help of the compulsory birth registry and the public health care system in Norway, the researchers have looked at the specific order and severity of hypertensive disorders of pregnancy throughout women's lifetime number of pregnancies.
Previous studies have concluded that having a hypertensive disorder of pregnancy doubles your risk of heart attack and stroke. Wyatt found instead that some people have severe risks compared to previous estimates, with almost 10-fold increased risk.
"These people at high risk have a rare pattern of more than one hypertensive disorder in their reproductive history, and they delivered their pregnancies early, which may indicate more severe conditions," says Wyatt.
Wyatt also found that some patterns on pregnancy histories that include hypertensive disorders are not associated with heart attack and stroke at all.
"These people with little to no risk have the most common pattern of hypertensive disorders of pregnancy, only presenting with a hypertensive disorder in the first pregnancy, delivered on time without indications that there were serious problems or medical intervention, and going on to have later healthy pregnancies," she says.
"Previous analyses merging all pregnancy patterns of HDP into one variable may mask the true underlying risks of both low and high-risk mothers," Wyatt states.
Even people who only gave birth to one child were included as a unique pattern in the study, and it was consistently found that they have a higher risk of heart attack and stroke compared to people with more children. Beyond HDP, it's possible that other characteristics of reproductive history, like fertility, could also predict future CVD.
"Our study has added greater nuance to our understanding of hypertensive disorders of pregnancy, that while some may be related to cardiovascular disease, others may have other causes," says Wyatt.
There has recently been a push in the medical community to start screening and interventions for mothers who had a hypertensive disorder of pregnancy.
"This study adds to the evidence that CVD mortality cannot be predicted by a history of HDP alone but must be predicted in the context of multiple factors across our lifetime reproductive history," says Wyatt, and adds,
"This project has highlighted the greater need for research into hypertensive disorders of pregnancy, especially with a lens of every pregnant person's unique experience."
The research is published in the journal Paediatric and Perinatal Epidemiology.
More information: Sage Wyatt et al, Heterogeneity in the risk of cardiovascular disease mortality after the hypertensive disorders of pregnancy across mothers' lifetime reproductive history, Paediatric and Perinatal Epidemiology (2024). DOI: 10.1111/ppe.13059
Provided by University of Bergen







Post comments