
By Richard N. Fogoros, MD
Medically reviewed by Anisha Shah, MD
"Heart block" is a condition in which the heart's electrical signal is slowed down or stopped entirely as it moves from the upper cardiac chambers (the atria) to the lower cardiac chambers (the ventricles).
chombosan / iStockphoto
Heart block—also called atrioventricular block, or AV block—is one of the two major causes of bradycardia (slow heart rate). (The other major cause is sinus bradycardia).
Overview
In heart block, the heart's electrical impulses are partially or completely blocked as they attempt to travel from the atrial chambers of the heart to the ventricular chambers. Because these electrical impulses let the heart know when it is supposed to beat if heart block is severe enough it may slow the heart rate to dangerously low levels.1
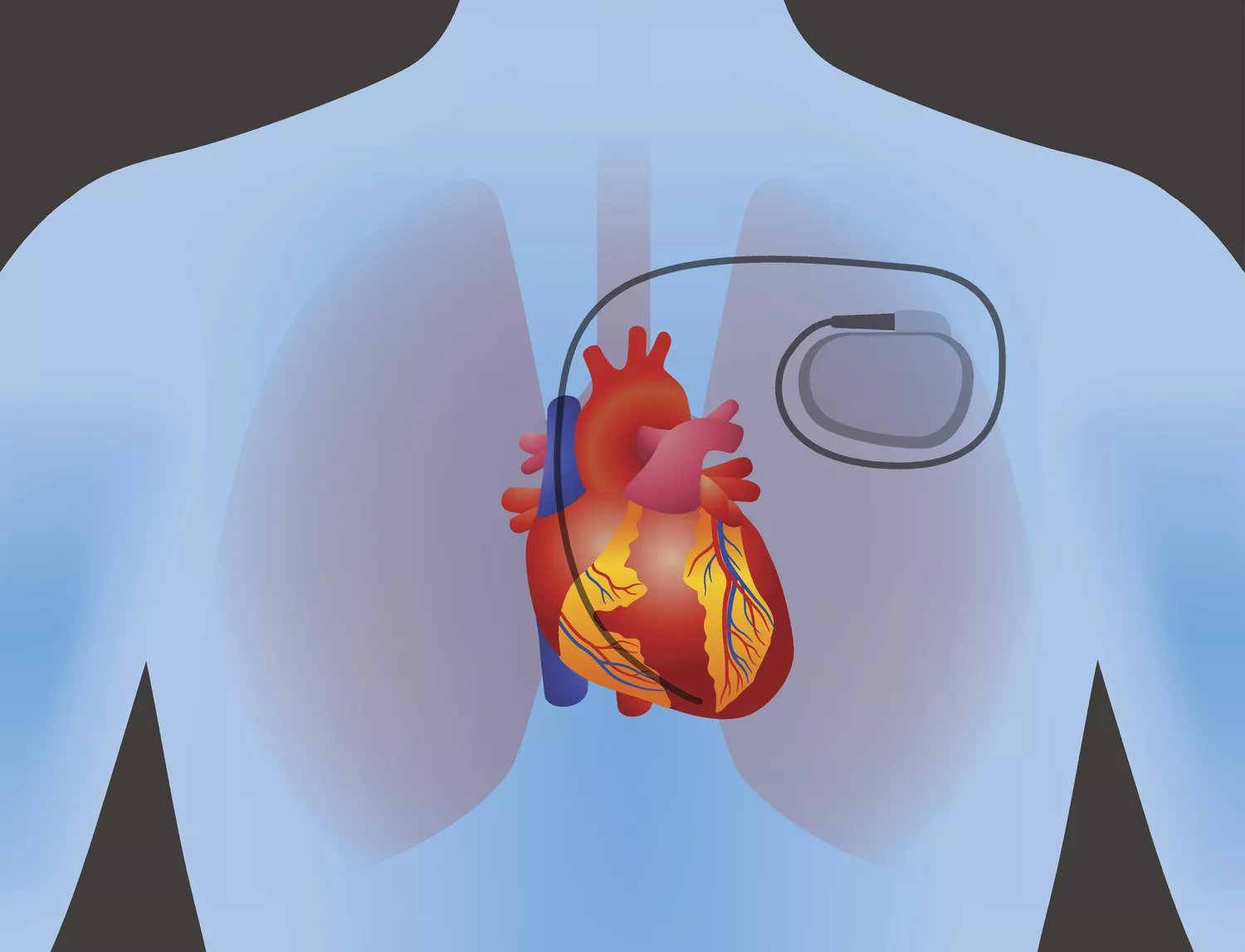
If you have heart block, the main question your healthcare provider will need to answer is whether you will need a pacemaker to prevent serious injury or death from an extremely slow heart rate. To answer this question, your healthcare provider will need to determine what is causing your heart block, and whether the heart block is transient or whether it is likely to persist or become even worse.
In making this evaluation, your healthcare provider will take into account the cause of your heart block, the symptoms you are experiencing from it, the degree of heart block (more on this below), and the specific location within your heart that is causing the block.
Causes of Heart Block
Brief episodes of heart block are not always dangerous or even abnormal. Transient heart block is often seen in young, healthy people who experience a sudden increase in the tone of their vagus nerves.
This increased vagal tone often happens with nausea, vomiting, or in response to pain, fright, or sudden stress. This form of heart block is not life-threatening and does not indicate any underlying problem with the heart's electrical system. It disappears immediately once the triggering event has subsided and almost never requires the insertion of a pacemaker.
On the other hand, heart block can also occur with various cardiac diseases, especially coronary artery disease, heart failure, or myocarditis. There are also congenital forms of heart block.
In general, when a heart block is produced by heart disease, there is likely to be a permanent disorder of the cardiac electrical system. This kind of heart block often gets worse over time, so pacemakers are often required.2
Symptoms of Heart Block
Depending on its severity, heart block may produce a range of symptoms, from none at all to dizziness, syncope (loss of consciousness), or even death.
If heart block is producing symptoms—especially dizziness or syncope—then treating it with a pacemaker is usually required. The exception to this general rule is when the heart block is known to be transient—for instance, when it is due to a temporary increase in vagal tone.
Heart block that is not producing any symptoms whatsoever usually does not require a pacemaker, unless it is one of the kinds of heart block that is very likely to get worse over time. 3
Degree of Heart Block
Heart block is categorized by healthcare providers into one of three "degrees." Your healthcare provider can determine the degree of your heart block with an electrocardiogram (ECG). The higher the degree of block, the more dangerous the heart block is likely to be.
First-degree block means that each cardiac impulse eventually makes it from the atria to the ventricles, but the conduction of the impulse is slowed.
Second-degree block means that some of the impulses are successfully conducted to the ventricles, but some are not.
Third-degree block means that all of the electrical impulses are blocked, and none of them are reaching the ventricles. Third-degree heart block is also referred to as "complete heart block."
In a person with third-degree heart block, survival depends on the existence of extra pacemaker cells located below the site of the block. These subsidiary pacemaker cells generate their own electrical impulses, usually at a very slow rate, which at least allows the heart to keep on beating.
The heart rhythm produced by these subsidiary pacemaker cells is called an "escape rhythm." An escape rhythm, while life-saving, is often unreliable for prolonged periods of time.
In general, the higher the degree of heart block, the more likely the need for a pacemaker. Pacemakers are almost always required with third-degree block, often with second-degree block, but only rarely with the first-degree block.
Location of Heart Block
During the normal heart rhythm, the heart's electrical impulse must pass across the junction between the atria and the ventricles (the AV junction). This AV junction consists of two structures:
The AV node
The His bundle (which can be thought of as a compact “cable” of fibers that conduct electrical impulses from the AV node to the ventricles)
In determining the severity of the heart block, it is important to know where in the AV junction the block is occurring. Specifically, is the block within the AV node, or is it in the His bundle (or the bundle branches which arise from the His bundle)?
In most cases, the healthcare provider can determine the location of the heart block simply by examining the ECG. Sometimes, however, an electrophysiology study is needed to precisely localize the area of the block.
Heart block that occurs within the AV node (so-called "proximal" heart block) is usually pretty benign and often does not require a permanent pacemaker. When the block is occurring within the AV node, subsidiary pacemaker cells in the AV node just beyond the site of the block often take over the rhythm of the heart. This is called a "junctional escape rhythm."
On the other hand, with a "distal" heart block, the block occurs in or below the His bundle. Any subsidiary pacemaker cells in a person with a distal heart block can only be located in the bundle branches or the ventricles. The resulting heart rhythm is called a “ventricular escape rhythm.” Ventricular escape rhythms are not only extremely slow, but they also are also notoriously unreliable. The presence of a ventricular escape rhythm is usually considered a medical emergency.
Distal heart block tends to worsen over time. So even in cases where it is currently causing an only first or second-degree block, distal heart block is considered dangerous, and virtually always requires treatment with a pacemaker.
Sources
Cleveland Clinic. Heart Block. Last Reviewed on July 18, 2019.
Kashou AH, Goyal A, Nguyen T, et al. Atrioventricular Block. In: StatPearls. July 4, 2019.
National Heart, Lung, and Blood Institute. Conduction Disorders.
Additional Reading
Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2018.
Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Circulation 2008; 117:e350.

By Richard N. Fogoros, MD
Richard N. Fogoros, MD, is a retired professor of medicine and board-certified in internal medicine, clinical cardiology, and clinical electrophysiology.





Post comments