
by American Society for Microbiology
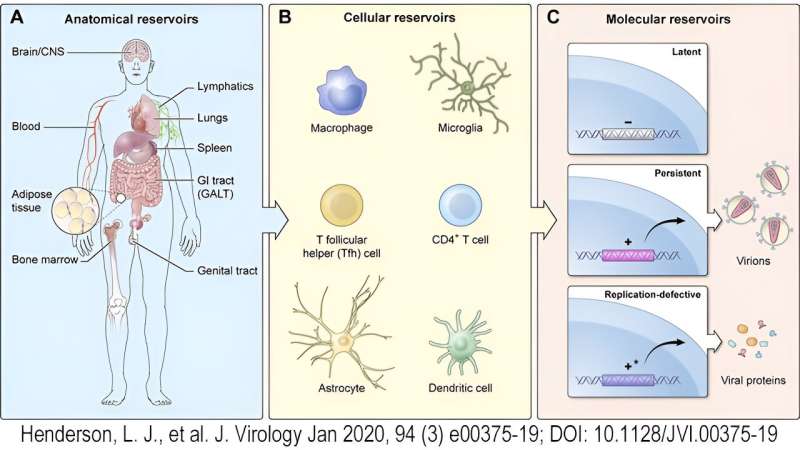
HIV-1 Latency can occur in a number of different anatomical sites, as well as multiple immunological cell types. Latent virus is not detectable by the host immune system or responsive to ART; however, upon reactivation, the virus can be expressed and perpetuate infection. Credit: https://jvi.asm.org/content/94/3/e00375-19
A 36-year-old Brazilian man made headlines around the world in 2020 for being the first person to be putatively cured of human immunodeficiency virus (HIV) using an easily accessible and well-tolerated drug cocktail.
The HIV treatment landscape is heart-breakingly littered with patients preliminarily declared cured who ultimately saw their infections return. And sadly, that was ultimately true for this patient's treatment too. But, his case sowed cautious hope that maybe, just maybe, we are one step closer on the road to a cure.
What was especially exciting about the São Paulo Patient's case (as he's being called to protect his privacy) was that he was the only person to have been reportedly cured of HIV without an arduous bone marrow transplant (BMT). The only other 2 reported HIV cures, the Berlin Patient and the London Patient, had progressive malignancies that provided the opportunity to use BMT to dually treat both their cancer and their HIV.
BMT is no small endeavor. It involves wiping out the resident immune system (including, hopefully, all HIV-infected cells) and re-seeding it with healthy donor cells. It's a slash-and-burn approach, roughly equivalent to destroying and re-growing an organ. The Berlin and London patients were seeded with cells from donors who lacked the primary cell-surface co-receptor for HIV, C-c chemokine receptor type 5 (CCR5), meaning their 'new' immune system would be protected from R5-tropic viral infection.
Bone marrow transplant, being costly, risky, and intensive, is not a scalable option for the millions living with HIV, particularly in low-resource areas. An accessible drug cocktail, however, might just be.
HIV latency and the trouble with finding a cure
Despite the resounding success of antiretroviral therapy (ART), which corrals viral replication to low or undetectable levels in most adherent individuals, a true cure has been elusive for HIV. This is due to HIV latency, in which the virus hides in an inactive state in the genomes of long-lived host cells (such as resting memory T cells) where it evades immune clearance. Since ART acts on viral replication machinery, latent virus that is not actively replicating also evades antiretroviral drugs.
Scientists have recognized for years that latency is one of the primary challenges to overcome in the quest for a cure. Although long-lived resting central memory CD4+ T cells are a primary reservoir for latent HIV, it has also been known to establish latent infection in various other CD4+ T cell compartments, macrophages and even dendritic cells.
Latently infected cells may also hide in privileged or complex anatomical sites, such as the central nervous system, genital tract or gut-associated lymphoid tissue. In addition to complicating cure strategies, these reservoirs make it difficult to determine whether virus remains in the body, as many clinical studies test for proviral DNA in only the circulating immune cells that can be collected in a standard blood draw. What's more, much like cancer, it only takes one missed reservoir cell to reignite the infection.
In light of these challenges, many research teams are investigating molecular methods to coax HIV out of hiding and into view of the immune system. Driving expression of HIV is desirable because it makes the virus a target for destruction by normal immunological mechanisms, and the hope is that doing so will result in clearance of the latent reservoir.
Many trials using latency reversal agents (LRAs) have been pursued in recent years. These methods must walk the tricky balance of causing enough immune activation to release the entirety of the hiding proviral reservoir without over activating the immune system and causing inflammation in fragile sites, such as the brain. Unfortunately, one in vitro study showed that even if 100% of a subset of T cells are activated, some perfectly competent proviruses remain tucked away.
This suggests that cellular activation alone as a latency reversal strategy may not be sufficient to clear the viral reservoir.
Another focus has been zeroing in on the epigenetics of HIV latency: in other words, trying to remove transcriptional inhibition so that HIV can be expressed without otherwise over-activating the immune system.
A few tactics in this arsenal include transcription factors, such as nuclear factor kappa-light-chain-enchancer of activated B cells (NF-κB) or nuclear factor of activated T cells (NFAT), that promote viral expression, histone deacetylase (HDAC) inhibitors, which help relax the DNA so it can be transcribed, and methyltransferase inhibitors, which remove inhibitory enzyme activity in the HIV promoter.
Gene editing strategies have also been attempted. These focus on altering cell genomes, rather than driving viral expression, to encourage the immune system to naturally eliminate infected cells. Preclinical studies in animal models that disrupt the CCR5 co-receptor gene using zinc-finger nucleases show promising protection against HIV, but so far are not curative. Subsequent clinical trials assessing this method have been safe and sufficient to reduce HIV viremia, but they have not ultimately resulted in an HIV cure.
Clustered regularly interspaced short palindromic repeats (CRISPR)-Cas9 gene editing approaches have also been investigated extensively preclinically, with some success in a combination approach that targeted the HIV gag gene and eliminated viral detection in multiple body compartments of murine models.
This therapy was successful in 2 out of 7 mice, however, and has not yet been clinically tested. A recent human case study of CRISPR disruption of CCR5 in an HIV patient with comorbid leukemia showed only limited engraftment. Nonetheless, gene editing strategies continue to be promising approaches for future HIV research.
A combination of strategies is likely to be the name of the game when it comes to eliminating wiley HIV reservoirs. Regardless of the many HIV clearance strategies that have been investigated, none have struck quite the right balance in the clinic of viral clearance-to-regimen tolerability in their own right. However, there is still much promise for linking several strategies together, and that is exactly what came through for the São Paulo Patient.
The São Paulo Patient's Treatment
Ricardo Diaz, M.D., and his team at the Federal University of São Paulo wanted to compare a variety of combination therapies for the elimination of HIV, from simply intensifying ART to using various LRAs with or without immunological enhancement. They recruited 30 HIV+ male volunteers who had demonstrated viral control for at least 2 years on ART, and randomized the men into 6 groups of 5. Each group received various combination strategies as follows:
The control group persisted on their normal ART regimen.
Another group received their normal ART regimen with 2 additional drugs, dolutegravir and miravoc, the latter of which has been shown to act as a latency reversal agent (LRA).
In the third group, Diaz gave enhanced ART and the HDAC inhibitor nicotinamide (vitamin B3) as an enhanced effort to coax HIV out of latency.
Group 4 received enhanced ART with the gold dust auranofin, which has shown promise with its redox properties in the treatment of other diseases.
Group 5 received a partially intensified ART (just dolutegravir), followed by a therapeutic dendritic cell vaccine to boost anti-HIV immunity.
Finally, Group 6 received the gamut: partially intensified ART, nicotinamide as an HDAC inhibitor, the gold dust auranofin and the therapeutic vaccine.
The São Paulo Patient hailed from Group 6.
He maintained undetectable viral DNA after cessation of all ART for nearly a year and a half. Even still, it wouldn't be unprecedented for his HIV to return. What gave Diaz hope, according to an interview with journalist Terri Wilder, was that his HIV antibody levels were declining.
This suggested that there was no antigen (HIV) to stimulate their production, and is reflective of what was observed in the other 2 cured patients. However, low or undetected antibody has also been observed in HIV+ infants who receive ART before 6 months of age, including the 'Mississippi baby' whose infection returned after years of remission.
Importantly, the São Paulo Patient was the only one of his group of 5 to achieve HIV remission, even though others in his group cleared proviral DNA below detection limits by the end of the study.
This whispers strong caution to even the most buoyant excitement, and hints at possible exceptionality that the São Paulo Patient may have had. Did he begin ART early after his diagnosis? Did he have an immunological profile that favored viral control? Did he get initially lucky and have a larger share of his HIV rooted out of hiding?
We at least know that prior to the clinical trial, he did not demonstrate special characteristics of 'elite control,' or the ability to spontaneously control HIV infection without the use of ART. This amazing capability of HIV elite controllers to suppress the virus without ART is not fully understood, but appears to be a facet of genetic advantage of the immune system—especially the human leukocyte antigen (HLA) allele—or perhaps the sequestration of proviral DNA to non-transcribed regions of the genome, among other possibilities.
However, the São Paulo Patient was on ART and had experienced blips of viremia, meaning that he was not likely an elite controller.
Time and research will continue to illuminate our understanding. Diaz and his team have secured funding for a second, larger clinical trial following up on the same treatment. But for now, and for this 34th Annual World AIDS Day, we celebrate the possibility of hope, the promise of progress and one man's exciting success in the fight against HIV.
*The Berlin Patient, Timothy Ray Brown, passed away on Sept. 29, 2020 of his leukemia, though he remained cured of HIV for the remainder of his life.
Provided by American Society for Microbiology







Post comments