
by Queen Mary, University of London
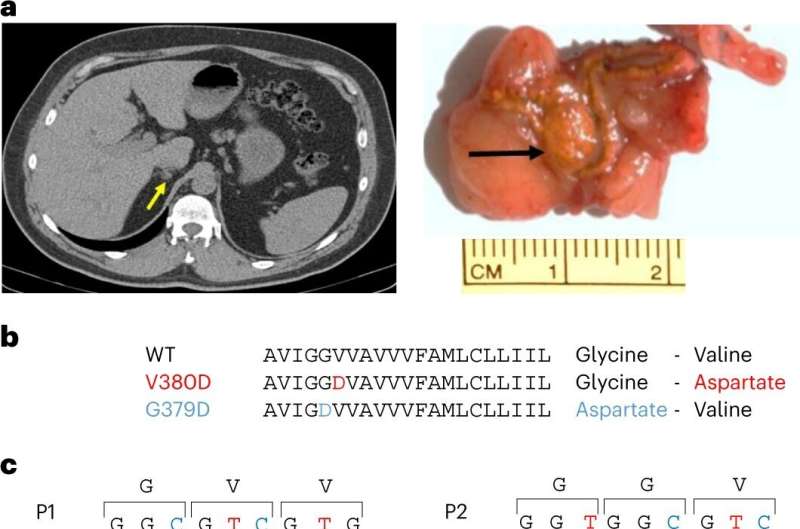
Discovery of CADM1 somatic mutations in APAs. a, APA of patient P1 as seen on CT scan (yellow arrowhead) and in adrenal tissue (black arrowhead). The axial CT image of patient P1’s adrenal identified a 13 × 7 mm right adrenal nodule. Macroscopic view of 5-mm adrenal slices reveals the solitary adenoma. IHC imaging of CADM1-mutant APAs from patients P1–P5 are shown in Extended Data Figs. 1 and 2. b, Affected protein residues in the TM domain of CADM1. Protein sequence showing the mutations in adjacent amino acids. c, Sanger sequencing chromatograms of the two CADM1 somatic mutations found in APAs (P1–P5). The two somatic mutations in CADM1 translate to a p.Val380Asp (V380D) and p.Gly379Asp (G379D) mutant CADM1. The somatic mutations were found in neither the blood (of P2) nor the adjacent adrenal gland gDNA (of P1). cDNA sequence of APA from patient P1 suggests expression of both WT and mutant CADM1 protein in the adenoma. Credit: Nature Genetics (2023). DOI: 10.1038/s41588-023-01403-0
Researchers have found that the cause of a common type of high blood pressure originates in a tiny benign nodule, present in one-in-twenty people with hypertension. The nodule produces a hormone, aldosterone, that controls how much salt is in the body. The new discovery is a gene variant in some of these nodules which leads to a vast but intermittent overproduction of the hormone.
Writing in Nature Genetics, researchers describe that the newly-discovered gene variant causes several problems, which makes it hard for doctors to diagnose some patients with hypertension. Firstly, the variant affects a protein called CADM1 and stops cells in the body from "talking" to each other and saying that it is time to stop making aldosterone.
Also an issue for doctors is the fluctuating release of aldosterone throughout the day, which at its peak causes salt overload and hypertension. This fluctuation explains why patients with the gene variant can elude diagnosis unless they happen to have blood tests at different times of day.
The researchers also discovered that this form of hypertension could be cured by unilateral adrenalectomy—removing one of the two adrenal glands. Following removal, previously severe hypertension despite treatment with multiple drugs disappeared, with no treatment required through many subsequent years of observation.
Fewer than 1% of people with hypertension caused by aldosterone are identified because aldosterone is not routinely measured as a possible cause. The researchers are recommending that aldosterone be measured through a 24-hour urine test rather than one-time blood measurements, which will reveal more people living with hypertension but going undiagnosed.
The initial patient in this study was detected when doctors noticed fluctuation in his hormone levels during his participation in a clinical trial of treatments for difficult hypertension.
In most people with hypertension, the cause is unknown, and the condition requires lifelong treatment by drugs. Previous research by the group at Queen Mary had discovered that in 5-10% of people with hypertension the cause is a gene mutation in the adrenal glands, which results in excessive amounts of aldosterone being produced.
Aldosterone causes salt to be retained in the body, driving up the blood pressure. Patients with excessive aldosterone levels in the blood are resistant to treatment with commonly used drugs for hypertension, and at increased risk of heart attacks and strokes.
Professor Morris Brown, co-senior author of the study and Professor of Endocrine Hypertension at Queen Mary University of London, said, "In the 900th anniversary of Barts Hospital, this story illustrates benefits from the virtuous circle of science and medicine. Most patients consent to our undertaking non-routine molecular analyses of their surgical samples, from which we discover how their hypertension was caused, and how to cure it in future patients.
"Because the aldosterone nodules in this study were so small, we are now investigating whether momentary cauterization of the nodule is an alternative to surgical removal of the whole adrenal gland."
More information: Wu, X. et al, Somatic mutations of CADM1 in aldosterone-producing adenomas and gap junction-dependent regulation of aldosterone production, Nature Genetics (2023). DOI: 10.1038/s41588-023-01403-0 www.nature.com/articles/s41588-023-01403-0
Journal information: Nature Genetics
Provided by Queen Mary, University of London







Post comments