
by Jordan Shaked, Yale University
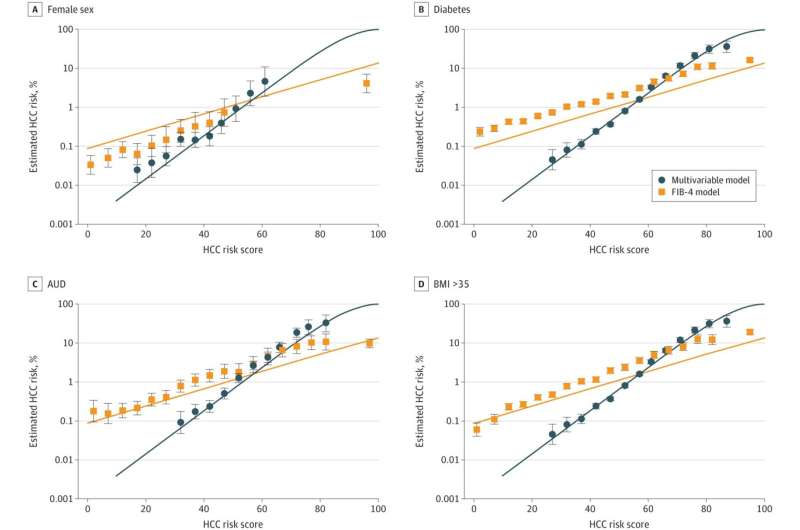
Ten-year risk of hepatocellular carcinoma (HCC). Credit: JAMA Network Open (2024). DOI: 10.1001/jamanetworkopen.2024.43608
Hepatocellular carcinoma, a type of liver cancer, is the sixth most common cancer worldwide and the third leading cause of cancer-related deaths. Screening efforts for this cancer focus on individuals diagnosed with viral hepatitis or those known to have irreversible liver scarring, or cirrhosis.
Due in part to increasing rates of obesity, another major risk factor is emerging, metabolic dysfunction-associated steatotic liver disease (MASLD), but factors associated with MASLD are not included in current screening practices.
In response, researchers at Yale and University of Pennsylvania have developed and validated a new risk score for hepatocellular carcinoma that considers these factors. Their work, "Risk Score for Hepatocellular Cancer in Adults Without Viral Hepatitis or Cirrhosis" was published on November 6, 2024, in JAMA Network Open.
One of the principal investigators of this study, Tamar Taddei, MD, professor of medicine (digestive diseases), emphasizes the need for improved screening guidelines for the disease. "Now that we can better treat viral liver diseases, we're increasingly observing hepatocellular carcinoma in patients with MASLD. This condition is harder to detect, and we're seeing liver cancer emerge in these patients even before cirrhosis develops. We want to understand the liver cancer risk in these populations."
The researchers conducted a cohort study using data from more than 6 million adults from the Veterans Health Administration (VA) electronic health records, excluding individuals with known hepatitis B or C infection or decompensated cirrhosis. They selected one random outpatient visit per person from 2007 to 2020, collecting information such as age, sex, race, body mass index, FIB-4 (an index that estimates liver fibrosis), diabetes, smoking, and alcohol use.
They followed these patients until a diagnosis of hepatocellular carcinoma, death, or the study's end. Of the 6,508,288 individuals studied, 15,142 developed hepatocellular carcinoma. The authors used the data they collected to create and validate a risk score for developing this deadly cancer.
While FIB-4 was the most important variable for identifying this unique liver cancer risk, the authors found that the other variables studied were informative too. For example, obesity and diabetes were independently and strongly associated with disease incidence. Janet Tate, MPH, ScD, one of the lead authors, ran the analyses that led to the development of a risk score.
"Conventional wisdom has been that you have to have a FIB-4 greater than 3.25 to be considered at high risk, but our work refutes this. Most of our hepatocellular carcinoma cases were in people who had FIB-4 lower than that," says Tate.
FIB-4 has previously been validated in populations with viral, alcoholic-associated, and steatotic liver diseases with varying diagnostic accuracy. Importantly, when developing their own liver cancer risk score, the authors broke FIB-4 into its component variables (AST, ALT, platelets, and age), and utilized continuous, rather than categorical, variables for their final model. Both of these helped the researchers strengthen their prediction model.
"I would encourage other statisticians or epidemiologists to not be afraid of continuous variables," says Tate. "Categorical variables may be easier to digest, but even if you have very fine categories, there's a loss of information."
The goal of this risk score is not to pinpoint one specific risk factor as most important but to calculate the cumulative effects of multiple factors that may contribute to hepatocellular carcinoma for a given individual, exemplifying precision medicine.
The authors report that the risk score has a higher sensitivity and positive predictive value compared to FIB-4 alone, and additionally identify a gradient of risk among those with specific FIB-4 scores. "This work puts all the risk factors together, coming up with a single score, from zero to a hundred, that everybody can get their heads around," says Tate.
Another principal investigator of the study, Amy Justice, MD, Ph.D., C.N.H. Long Professor of Medicine (general medicine) at Yale School of Medicine, and professor of public health (health policy) at Yale School of Public Health, hopes that this study may help patients understand the different modifiable risk factors for liver disease.
"Factors such as smoking and obesity not only contribute to the development of cardiovascular disease but also to liver disease," says Justice. "Recognition and modification of these risk factors is essential to improving health outcomes."
The authors hope to validate their risk score in settings beyond the VA. "There is a perception that the VA data may not be generalizable outside of its context. However, based on my extensive experience in predictive modeling with HIV, our collaborations with various other cohorts have consistently shown that findings identified in the VA are applicable in broader populations," says Justice.
The risk score developed in this study uses variables commonly and easily tested in primary care settings. "This clinical score provides primary care clinicians with a straightforward tool to assess whether to be concerned about liver cancer or liver disease," says Taddei. "The earlier we in specialty care receive these consultations, the more effectively we can address the risk factors for liver cancer. If this score prompts clinicians to consider liver health, I consider it a success."
More information: Ysabel C. Ilagan-Ying et al, Risk Score for Hepatocellular Cancer in Adults Without Viral Hepatitis or Cirrhosis, JAMA Network Open (2024). DOI: 10.1001/jamanetworkopen.2024.43608
Journal information: JAMA Network Open
Provided by Yale University





Post comments