
by Brigham and Women's Hospital
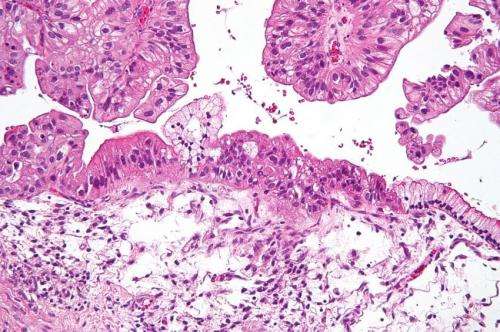
Intermediate magnification micrograph of a low malignant potential (LMP) mucinous ovarian tumour. H&E stain. The micrograph shows: Simple mucinous epithelium (right) and mucinous epithelium that pseudo-stratifies (left - diagnostic of a LMP tumour). Epithelium in a frond-like architecture is seen at the top of image. Credit: Nephron /Wikipedia. CC BY-SA 3.0
Investigators from Brigham and Women's Hospital and Dana-Farber Cancer Institute are leveraging the power of artificial intelligence to develop a new technique to detect ovarian cancer early and accurately. The team has identified a network of circulating microRNAs - small, non-coding pieces of genetic material - that are associated with risk of ovarian cancer and can be detected from a blood sample. Their findings are published online in eLife.
Most women are diagnosed with ovarian cancer when the disease is at an advanced stage, at which point only about a quarter of patients will survive for at least five years. But for women whose cancer is serendipitously picked up at an early stage, survival rates are much higher. Currently, no FDA-approved screening techniques exist for ovarian cancer, making it challenging to diagnose the disease early in either women with a genetic predisposition for the disease or in the general population.
Ovarian cancer is relatively rare compared to other benign gynecological conditions such as ovarian cysts. But early detection tests, such as ultrasound or detection of the protein CA125, have a high false positive rate for ovarian cancer. And clinical trials have found that when these tests are used to try to detect early-stage ovarian cancer, they do not have a meaningful impact on survival rates. The Dana-Farber and BWH team sought a tool that would be more sensitive and specific in detecting true cases of early-stage disease.
The team looked at a set of molecules called microRNAs - non-coding regions of the genome that help control where and when genes are activated.
"microRNAs are the copywrite editors of the genome: Before a gene gets transcribed into a protein, they modify the message, adding proofreading notes to the genome," said lead author Kevin Elias, MD, of BWH's Department of Obstetrics and Gynecology.
"This project exemplifies the synergy of the two institutes DFCI and BWH and the power of clinicians working closely with lab-based scientists. My lab has been working on miRNAs for a decade and when Kevin came to us with the patient samples, it was a no-brainer to initiate this project" said the senior author Dipanjan Chowdhury, PhD, Chief of the Division of Radiation and Genomic Stability in the Department of Radiation Oncology at DFCI.
In the lab, Elias and Chowdhury and their colleagues determined that ovarian cancer cells and normal cells have different microRNA profiles. Unlike other parts of the genetic code, microRNAs circulate in the blood, making it possible to measure their levels from a serum sample. The team sequenced the microRNAs in blood samples from 135 women (prior to surgery or chemotherapy) to create a "training set" with which to train a computer program to look for microRNA differences between cases of ovarian cancer and cases of benign tumors, non-invasive tumors and healthy tissue. Using this machine-learning approach, the team could leverage large amounts of microRNA data and develop different predictive models. The model that most accurately distinguished ovarian cancer from benign tissue is known as a neural network model, which reflects the complex interactions between microRNAs.
"When we train a computer to find the best microRNA model, it's a bit like identifying constellations in the night sky. At first, there are just lots of bright dots, but once you find a pattern, wherever you are in the world, you can pick it out," said Elias.
The team then tested this sequencing model in an independent group of 44 women to determine the accuracy of the test. Once the accuracy of the model was confirmed, the team deployed the model across multiple patient sample sets, using a total of 859 patient samples to measure the sensitivity and specificity of the model. The new technique was far better at predicting ovarian cancer than an ultrasound test. Whereas using ultrasound fewer than 5 percent of abnormal test results would be ovarian cancer, almost 100 percent of abnormal results using the microRNA test actually represented ovarian cancer. Finally, the group put their final model into practice, using the microRNA diagnostic test to predict the diagnoses of 51 patients presenting for surgical care in Lodz, Poland. In this population, 91.3 percent of the abnormal test results were ovarian cancer cases - a very low false positive rate. Negative test results reliably predicted absence of cancer about 80 percent of the time, which is comparable to the accuracy of a Pap smear test.
"The key is that this test is very unlikely to misdiagnose ovarian cancer and give a positive signal when there is no malignant tumor. This is the hallmark of an effective diagnostic test," said Chowdhury.
The team also looked for evidence of biological relevance for the distinguishing microRNAs. They found changes in the quantity of these microRNAs in blood samples collected before and after surgery, suggesting that the microRNA signal decreases after the cancerous tissue is removed. They also took actual patient samples and imaged the microRNAs in the cancerous cells, demonstrating that the serum signal was coming from the cancerous tissues.
To move the diagnostic tool out of the lab and into the clinic, the research team will need to verify how the microRNA signature changes over time as risk of ovarian cancer increases. To do so, they will need to use prospectively collected, longitudinal samples following women over time. They are particularly interested in determining if the tool will be useful for women at high risk of ovarian cancer as well as the general population.
More information: Kevin M Elias et al, Diagnostic potential for a serum miRNA neural network for detection of ovarian cancer, eLife . DOI: 10.7554/eLife.28932
Journal information: eLife
Provided by Brigham and Women's Hospital






Post comments