
by Dan Lea, Mayo Clinic
Credit: Pixabay/CC0 Public Domain
Your genes play a role in nearly all areas of your health. A gene is like an instruction manual for your body that tells your body how to function, develop and stay healthy. People have about 20,000 genes in their bodies.
"Many health conditions have a genetic link," says Breanna Mitchell, a genetic counselor at Mayo Clinic Health System in Eau Claire. "Genetic testing can help you and your health care team understand if you have an increased risk for developing certain conditions that are present in your family. If you are at risk, you may be able to take preventive measures to decrease your risk or undergo genetic testing to clarify your risk."
Here are nine common questions about genetic testing:
Do all types of cancers have a genetic component?
Most cancers are considered sporadic, meaning the cancer happens randomly or has environmental influences, such as smoking and lung cancer. About 25% of cancers are considered familial. This is when multiple members of a family are affected by cancer. These family members have some shared genetic factors in combination with shared environmental factors that lead to the development of these cancers.
"About 10% of cancers are considered hereditary or have a single specific genetic component that can be tested and increase a person's risk for developing cancer," Mitchell says. "Genetic counseling and genetic testing can help determine which category a person's individual or family cancer falls into. It also can help estimate your risk for developing cancer."
What types of genes are examined during genetic testing?
You may have an increased risk for some health conditions, including some types of cancer, based on your genes. A genetic test looks for specific harmful gene changes, called mutations or pathogenic variants, that can cause you to develop a genetic condition. Gene changes are like spelling errors within your body's instruction manual.
Most genetic tests look for changes in a group of genes called a panel. However, testing may look for changes in a single gene when there is a known genetic mutation in your family. The most common genes typically thought of related to cancer risk are BRCA1 and BRAC2. These genes are associated with breast and ovarian cancer. It's known that changes in other genes can increase risk for these cancers, as well.
There also are gene panels that assess risk for other cancers, such as colorectal, pancreatic, prostate, liver, uterine and endometrial cancers.
Am I guaranteed to get cancer if I have a known gene?
No. Inheriting a harmful gene change means that you have an increased risk for cancer, but it does not guarantee that you will develop a cancer in your lifetime.
"If testing shows that you have an increased risk for cancer, you may need to be screened earlier or more often," Mitchell says. "For example, if you have a change in the BRCA gene that increases your risk for breast cancer, your care team will recommend that you have mammogram or MRI breast screenings beginning at a younger age or more frequently. The genetic counselor will explain your associated cancer risks and screening recommendations based on your genetic test results."
What criteria do I need to meet to have genetic testing completed?
Your health care team may recommend genetic testing based on guidelines established by the National Comprehensive Cancer Network (NCCN). These guidelines use factors such as your personal cancer history, family cancer history, ancestry or the presence of abnormal cells to determine if you qualify for genetic testing.
If you do not meet the NCCN guidelines, you can still pursue testing. Your health insurance may not cover any or all of the testing costs, so more out-of-pocket expenses to be tested are possible.
Can genetic testing help during cancer treatment?
If you are battling cancer, genetic testing can help your care team make recommendations for treatments and surgical procedures. For example, some cancers associated with genetic mutations respond better to certain types of chemotherapy treatments. Similarly, genetic testing can help you determine between a lumpectomy or a mastectomy when making surgical decisions about breast cancer. It also can affect the management of cancer risk over time.
"The results also can help other family members," Mitchell says. "Potentially, your children, siblings, nieces and nephews could have inherited the same gene mutation. Knowing this information can help them establish early screening schedules and make healthy decisions about their lives."
How can I prepare for a genetic testing consultation?
Gathering a detailed family health history is the most important thing to prepare for a genetic counseling appointment. Try to gather information about relatives, including types of cancer diagnosed, age of diagnosis, current age or age at death. Also find out if any relatives have perviously had genetic testing completed.
If no previous genetic testing has been performed, often the best person to be tested is the family member with cancer. That person is most likely to have a genetic change if there is one. If an affected family member is unavailable for testing due to death or lack of interest, an unaffected person can still be tested.
"Something else to think about before your consultation is the purpose of your test," Mitchell says. "Younger patients usually want to know their personal risk so they can do extra screening. Older patients who are cancer survivors may wish to gather information and share it with downstream family members so they are aware of harmful genetic changes they could have potentially inherited."
Am I only able to get cancer if I have the BRCA gene or one of these other genes?
A common misconception is that you have one of these genes or you don't. Everyone has the BRCA genes and these other genes associated with cancer risk. The role these genes play in the body is to prevent cancer from occurring.
It's when a harmful change occurs in one of these genes that causes it not to work like it should. This leads to the increased risk for cancer to develop.
People without these harmful changes can still develop cancer, but the risk is not as high as someone who has a hereditary predisposition.
Am I more likely to inherit something from a parent of the same sex as me? Or the parent that I most resemble?
No. Every person has two copies of every gene—one copy inherited from each parent. If a parent has a harmful genetic change in one copy of a gene, it is random which copy they will pass on to children.
Every child has a 50-50 chance of inheriting the typical copy or the changed copy, regardless of you or your parent's biological sex, or whether you more closely resemble one side of the family.
There is breast cancer on my dad's side of the family, I'm not at risk because my dad can't pass that on, right?
People often think that a heritable risk for some cancers, such as breast and ovarian cancer, can't be passed on from males. This is not true.
All people, regardless of biological sex, can carry a heritable risk factor for any type of cancer and can pass it on to any of their children.
"While you can't change your genes, you can control some aspects of your environment, such as diet and physical activity level, as well as alcohol and tobacco use," Mitchell says. "That's why it's still so important to live a healthy life, regardless of your personal and family genetic history."
Provided by Mayo Clinic
by Gillian Rutherford, University of Alberta
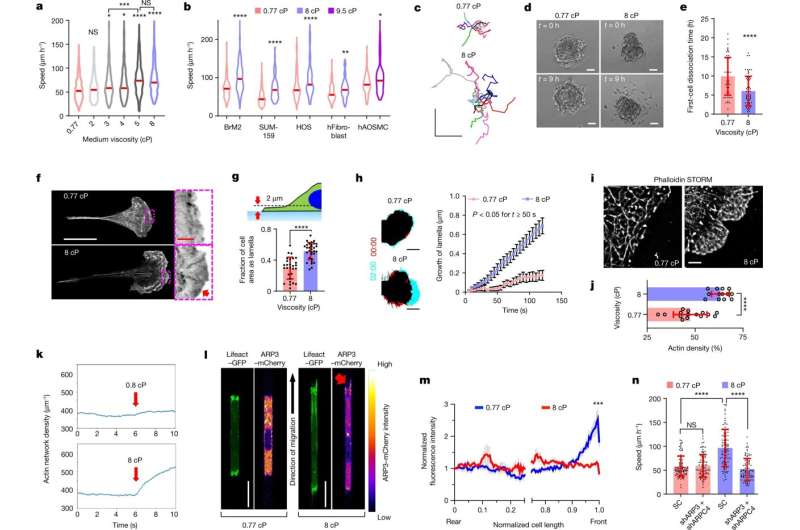
Viscosity enhances cell migration and promotes an ARP2/3-mediated dense actin network at the leading edge. a,b, Speeds of MDA-MB-231 cells (a) and other indicated cell types (b) inside confining channels at prescribed viscosities. The red lines represent the median of ≥69 cells from ≥3 experiments. c, Cell trajectories on 2D collagen-coated surfaces after 10 h. d, Cells disseminating from 3D spheroids. e, The time required for the first cell dissociation from each spheroid (n ≥ 53) from 3 experiments. f, Airyscan images of phalloidin stained cells on collagen-coated substrates. The red arrow indicates high F-actin staining along the cell edge. g, The fraction of cell-projected area with a Lifeact–GFP-rich lamella for n ≥ 28 cells from 3 experiments. h, The leading edge of Lifeact–GFP-expressing cells on collagen-coated surfaces at t = 0 min (red) and t = 2 min (cyan) (left). Right, leading-edge lamella growth in n ≥ 19 cells from 3 experiments. Data are the moving average ± s.e.m. P < 0.05 for all points t ≥ 50 s. Time is shown as min:s. i,j, STORM reconstruction (i) and density quantification (j) of F-actin for cells (n ≥ 13) on substrates from 2 experiments. k, The average actin density over time from 20 stochastic simulations. Viscous forces were applied at t = 6 s (red arrow) and maintained until the end of the simulation. l, Confocal images of cells expressing Lifeact–GFP and ARP3–mCherry in confinement. The red arrow indicates high ARP3 intensity at leading-edge protrusions at 8 cP. m, The relative ARP3–mCherry intensity along normalized cell length in confined cells. Data are the moving average ± s.e.m. for n = 21 cells from 4 experiments. ***P < 0.001 for all comparisons at normalized cell length > 0.96. The x axis is discontinued between 0.25 and 0.75 to highlight differences at the cell edges. n, Confined migration speeds of SC versus ARP3/ARPC4 double-knockdown cells (n = 90) from 3 experiments. For e, g, j and n, data are mean ± s.d. Unless otherwise indicated, statistical comparison was performed with respect to 0.77 cP. Statistical analysis was performed using Kruskal–Wallis tests followed by Dunn’s test (a and n), Mann–Whitney U-tests (BrM2 only) or unpaired t-tests after log-transformation (other cells) (b), unpaired t-tests (e, g and j) and two-way analysis of variance (ANOVA) followed by Šidák’s test (h and m). Scale bars, 250 μm (c), 50 μm (d), 25 µm (f, white), 3 µm (f, red), 10 µm (h), 2 µm (i), 20 µm (l). The cell model was MDA-MB-231 unless otherwise indicated. *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001. Credit: Nature (2022). DOI: 10.1038/s41586-022-05394-6
An international team of researchers has uncovered a new mechanism that enables cancer cells to move throughout the body, providing a potential new target to stop metastasis, which is responsible for 90 percent of cancer deaths.
In findings published in Nature, the team identifies that cancer cells move faster when they are surrounded by thicker fluids, a change that occurs when lymph drainage is compromised by a primary tumor.
"This is really the first time that the viscosity of the extracellular fluid has been looked at in detail," says John D. Lewis, professor and Bird Dogs Chair in Translational Oncology at the University of Alberta's Faculty of Medicine & Dentistry. "Now that we know that fluid viscosity signals cancer cells to move in a specific way, we can potentially use drugs to basically short-circuit that signaling pathway and encourage cancer cells to slow down, or even maybe to stop."
The Lewis lab was invited to join the project led by researchers at Johns Hopkins University, because of its expertise in imaging human cancer cells in real-time motion using the placenta-like chorioallantoic membrane from fertilized chicken eggs.
"I would say we're the world leaders in this type of imaging," Lewis says. "Our contribution to the work was to very precisely show that cancer cells change their gene expression when they encounter increased viscosity in the surrounding fluid and become more aggressive. And even when you bring the viscosity back down, these cells stay more aggressive."
"We then went on to show that when this signaling pathway is perturbed in cancer cells it changes their ability to escape the bloodstream and metastasize," Lewis says.
This is the third paper the international research team has published. Lewis credits Konstantin Stoletov, senior research associate, for the bulk of his team's work. He cautions that once a new therapeutic target is identified, it could take 10 to 15 years to develop and test a drug.
"But this is helping us build our understanding around how cancer cells move and it increases our chance of being successful with this whole approach," he explains.
More information: Kaustav Bera et al, Extracellular fluid viscosity enhances cell migration and cancer dissemination, Nature (2022). DOI: 10.1038/s41586-022-05394-6
Journal information: Nature
Provided by University of Alberta






Post comments